
Ultrasound images of early pregnancy
Contents of this page
- Bicornuate uterus with gestation sac
- Cornual pregnancy
- Another example of cornual or interstitial pregnancy
- Sonography of ruptured ectopic (tubal) pregnancy with pelvic hemorrhage
- HETEROTOPIC GESTATION
- Right ectopic pregnancy
- Scar Pregnancy (pregnancy in LSCS scar)
- LSCS scar Pregnancy- Case-2
- Anembryonic gestation
- Embryonic demise
- Subchorionic hematoma
- Abnormalities of yolk sac
- Double decidual sac sign
- 3D ultrasound- early fetal demise
- Cervical ectopic pregnancy
- abdominal ectopic pregnancy
- Live-ectopic-pregnancy
- low-implantation-gestation-sac
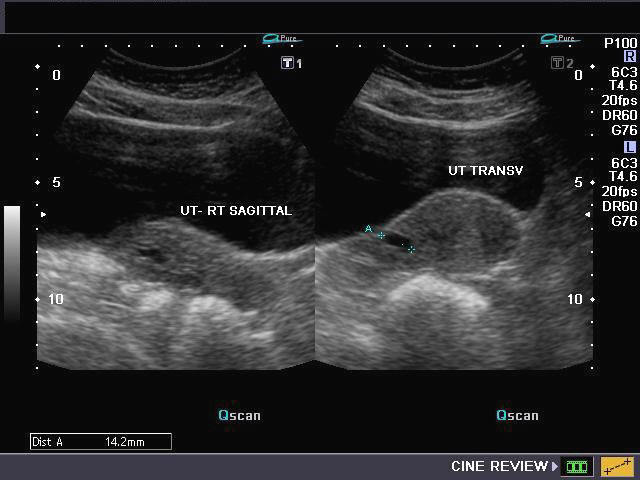
Bicornuate uterus with gestation sac

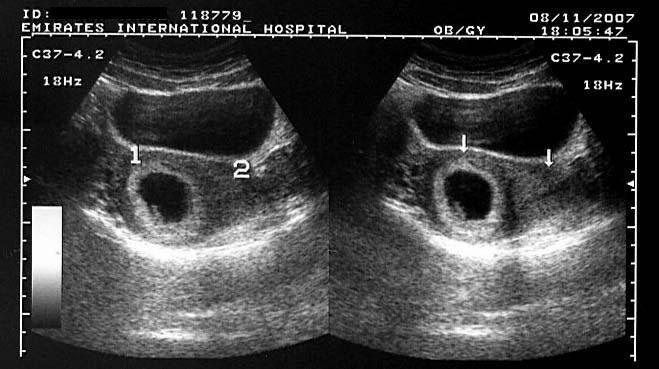
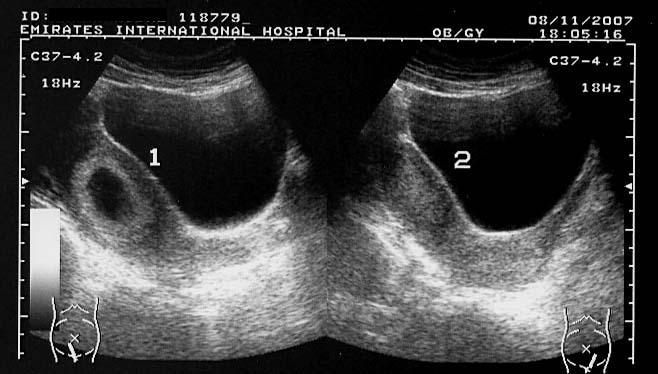
Pregnancy in one horn of uterus with two horns (cornu)
The above ultrasound images show a bicornuate uterus with a gestation sac in the right cornu (1). The empty left cornu (2) shows typical decidual changes of pregnancy. The 3rd image (right) is a sagittal section through each cornu.
Images courtesy of Dr. Ravi Kadasne, UAE.
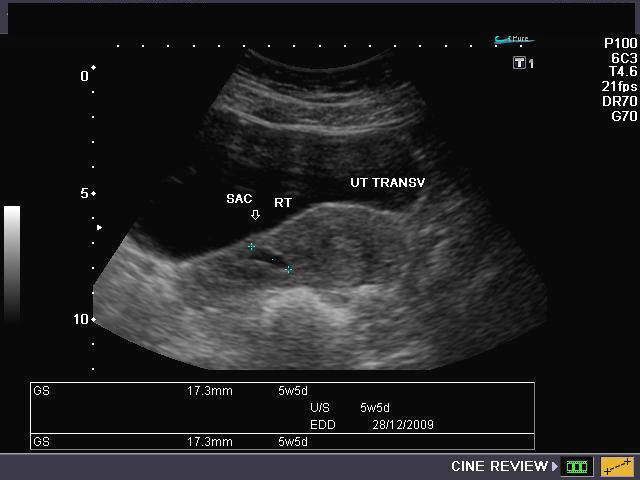
Cornual pregnancy

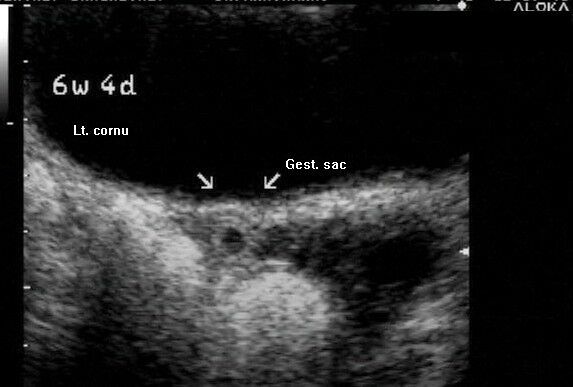
Sonography of the uterus shows a gestation sac of 6 weeks 4 days age, in the right cornu of the uterus. 3-D image of the uterus further confirms the findings. These ultrasound images are diagnostic of cornual pregnancy (a type of ectopic pregnancy). Ultrasound images courtesy of Dr. Latha Natrajan, Bangalore, India.
Reference:
1) http://www.thefetus.net/page.php?id=4 (free article)
2) http://www.jultrasoundmed.org/cgi/reprint/25/6/791.pdf (free article)
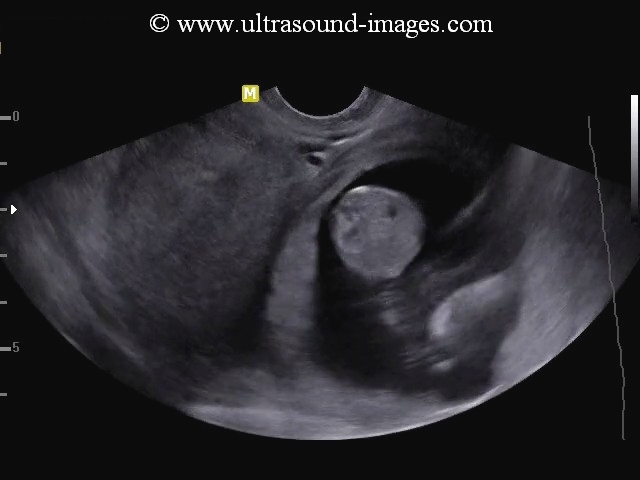
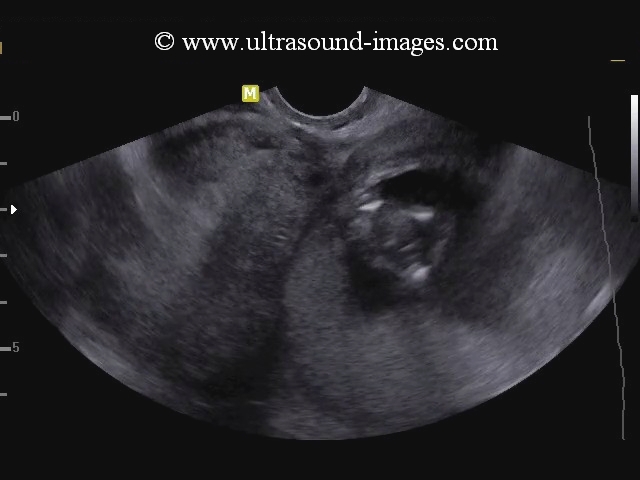
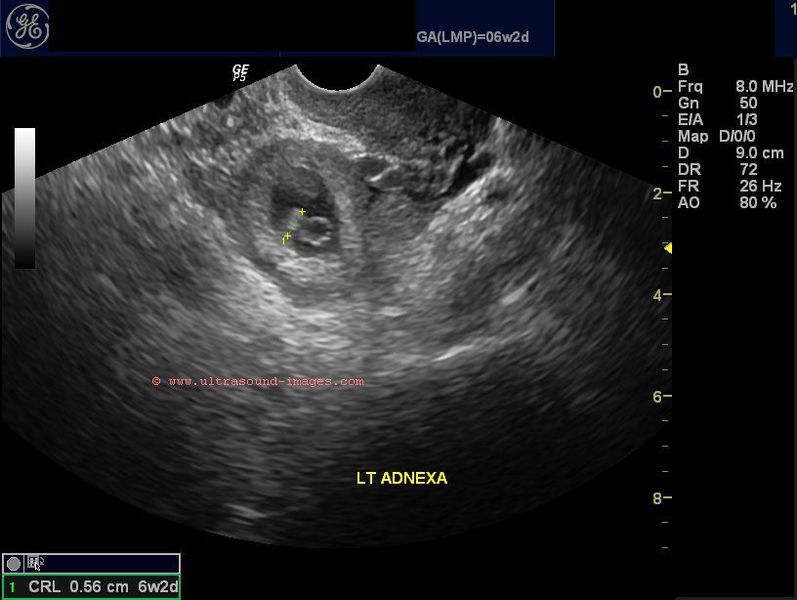
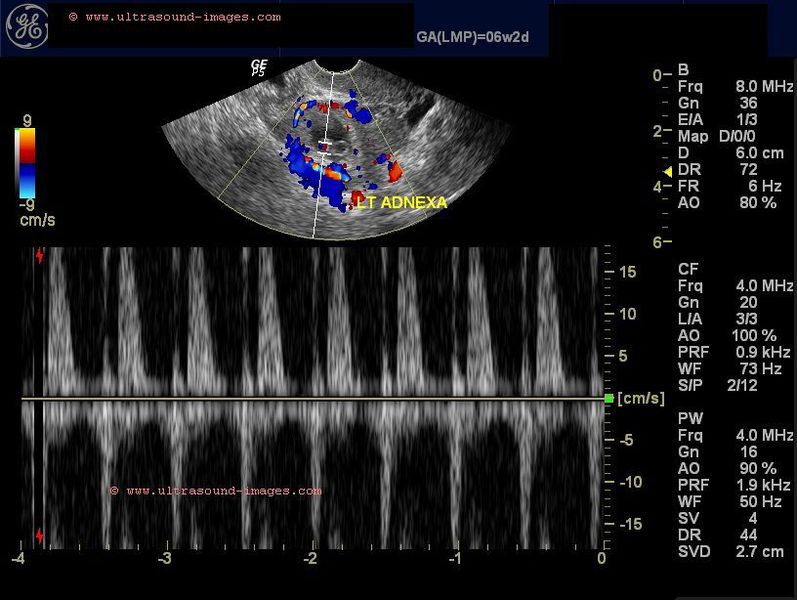
Another example of cornual or interstitial pregnancy
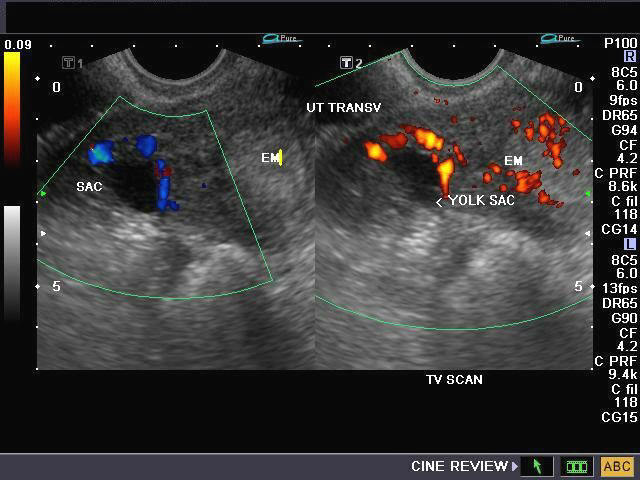
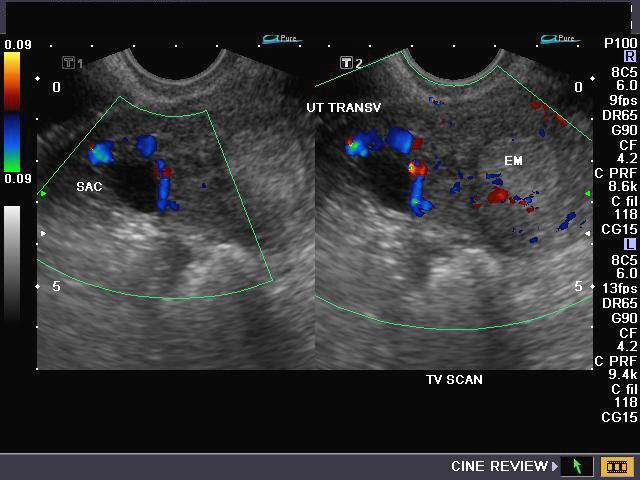
Sonography of cornual pregnancy
These ultrasound and color Doppler images show a gestation sac of 15mm. in the right cornu of the uterus (interstitial region of the fallopian tube). This patient had undergone IVF with embryo transfer 1.5 months back. The transvaginal Color / Power Doppler images (below) show a ring of vessels around the sac with a yolk sac (image lower right) within the gestation sac. No embryo is visualized at this stage. Note the empty endometrial cavity which shows decidual change. This pregnancy needs to be terminated with urgent surgical intervention.
Reference: http://www.medscape.com/viewarticle/557082_4
Download my E book for Amazon Kindle (download free Kindle reader for i Phone or Android)
Assorted ultrasound cases- by Joe Antony, MD
Sonography of ruptured ectopic (tubal) pregnancy with pelvic hemorrhage

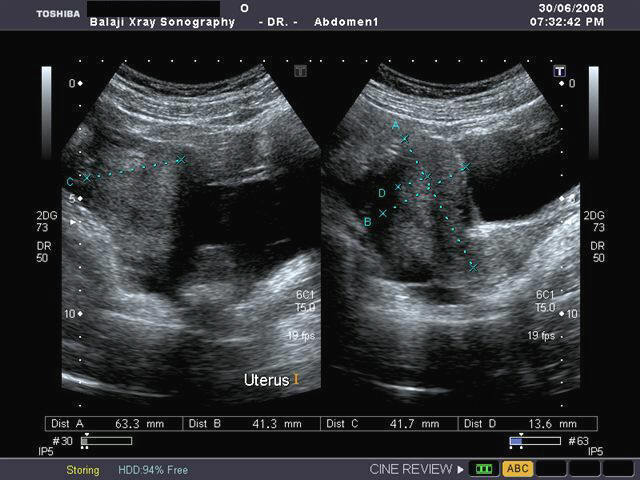

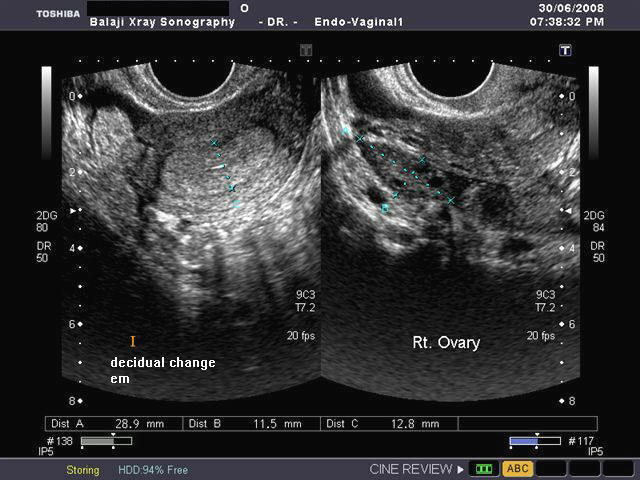
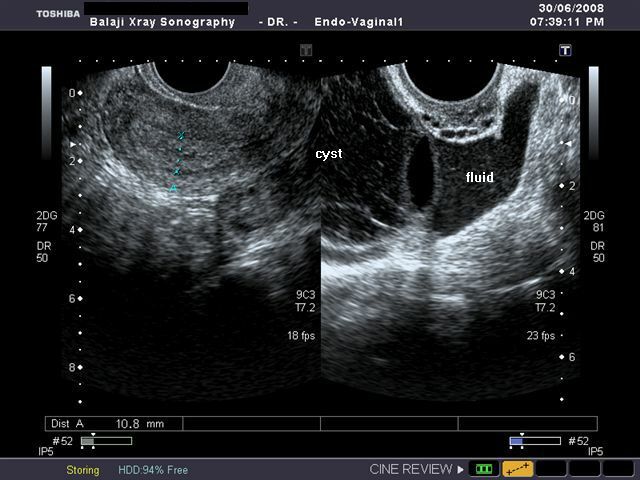
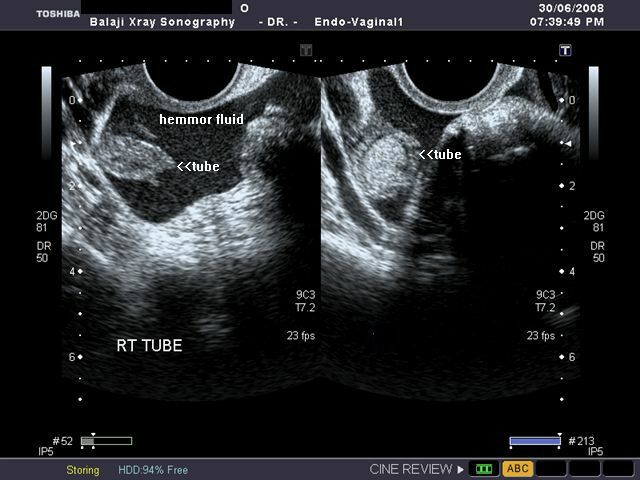
Sonography of the pelvis done on this female patient with pelvic pain and tenderness revealed: 1) enlarged (bulky) uterus with grossly thickened endometrium (decidual cast) of almost 15 mm. The uterus shows absence of any gestation sac. No pseudosac is seen. 2) Transvaginal scan of the pelvis shows a large collection of hemorrhagic fluid in the cul de sac 3) A right adnexal mass, presumably in the Right Fallopian tube is also seen. A left ovarian hemorrhagic cyst is also present.
These ultrasound images suggest a right tubal gestation with hematosalpinx with rupture of the Rt. Fallopian tube.
Ultrasound images courtesy of Dr. Gunjan Puri, Surat, India. The ultrasound machine used was the Toshiba Xario.
Heterotopic Gestation
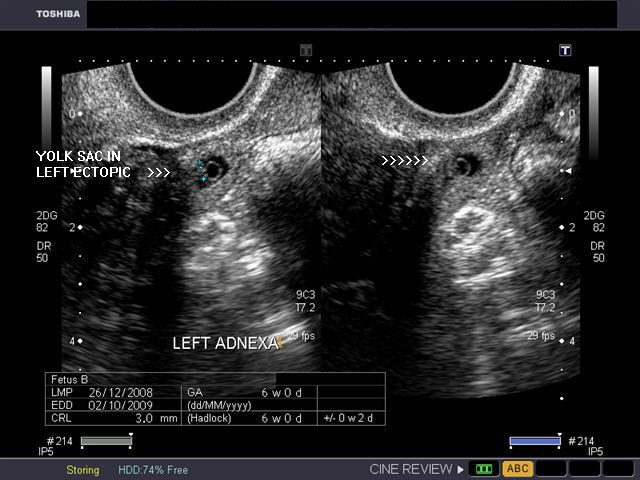
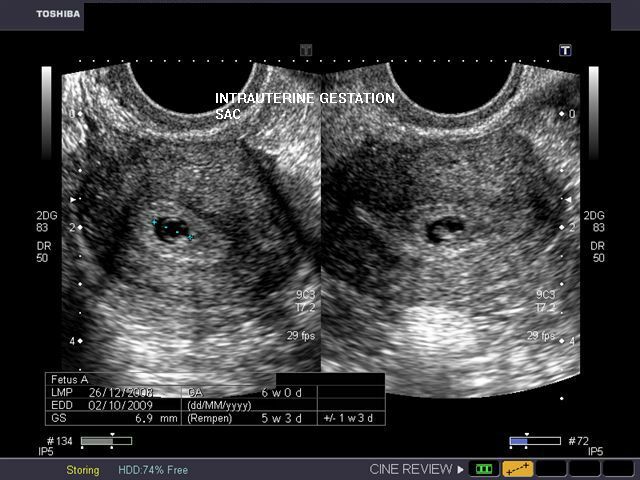

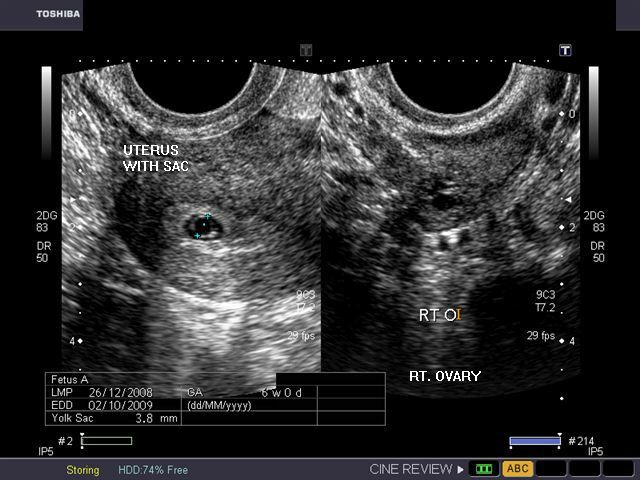
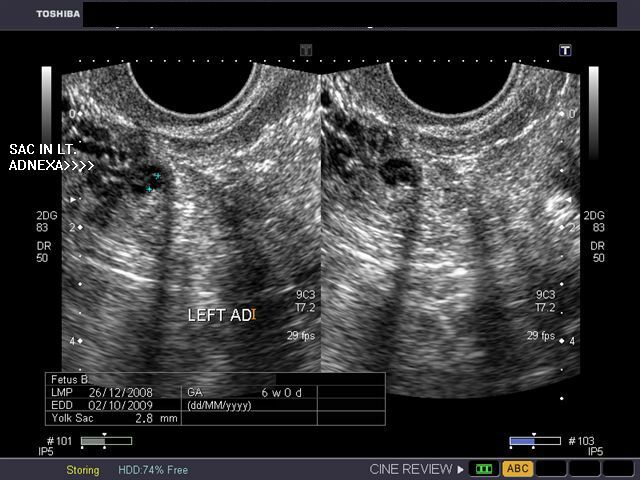
Transvaginal scan images
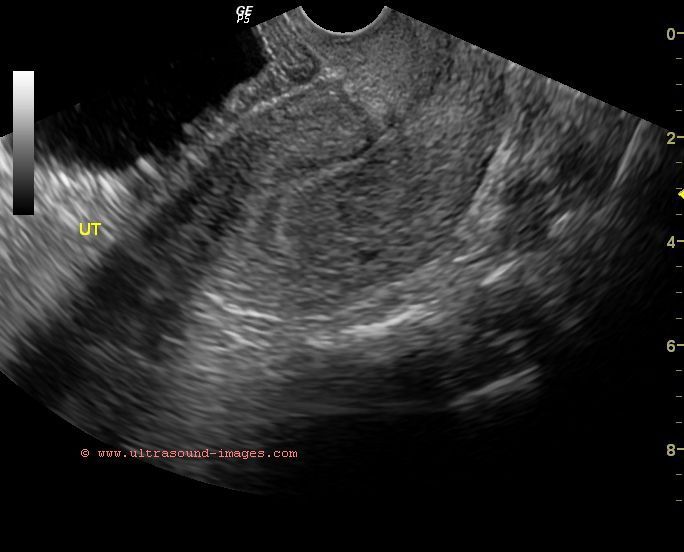
Transabdominal Scan

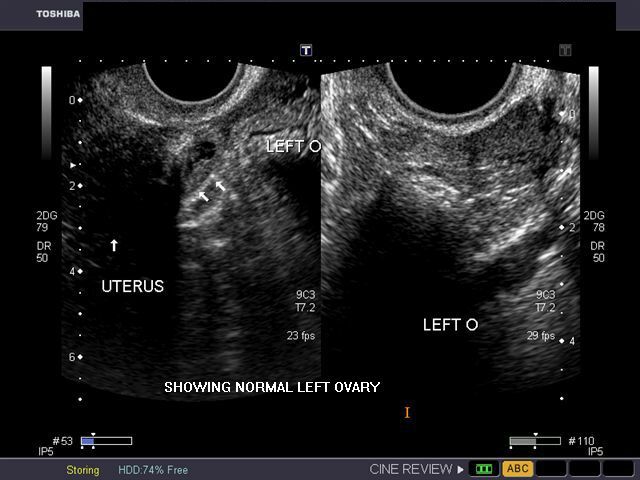
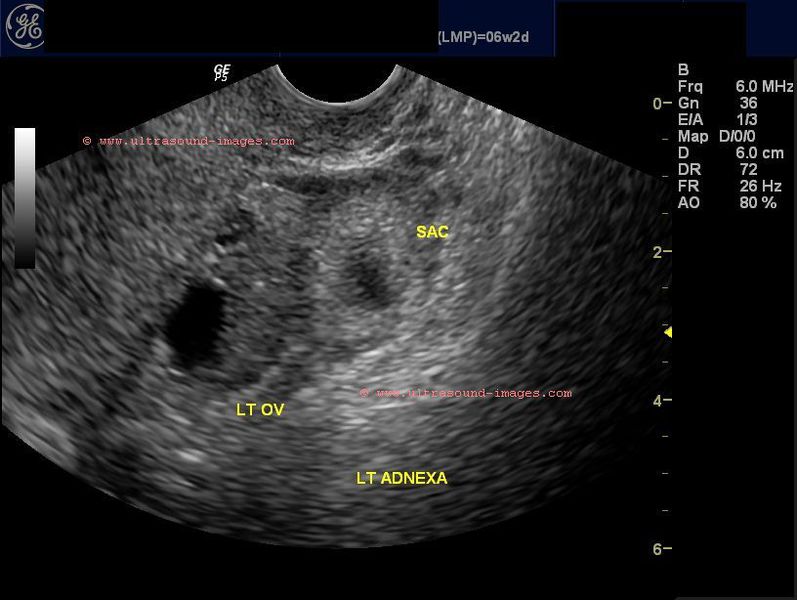
This patient presented with signs of early pregnancy with left sided pelvic pain and tenderness. Sonography of the pelvis shows an intrauterine pregnancy with a 6 weeks size embryo in the uterine cavity. There is also a coexistent left adnexal mass with a yolk sac like structure measuring 3 mm. and a possible embryo in the sac (6 weeks size). The right and left ovaries are separately identified on transvaginal ultrasound. These ultrasound images suggest heterotopic gestation (intrauterine embryo and a gestation sac in left adnexal region). Ultrasound images courtesy of Dr. Gunjan Puri, Surat, India. He used a Toshiba Xario ultrasound system here.
Reference: http://www.thefetus.net/page.php?id=3
Heterotopic gestation - case-2
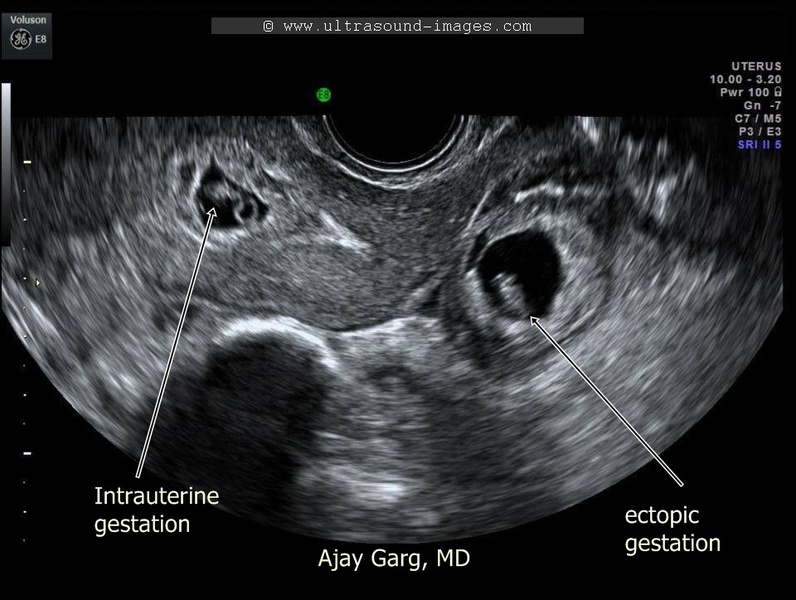
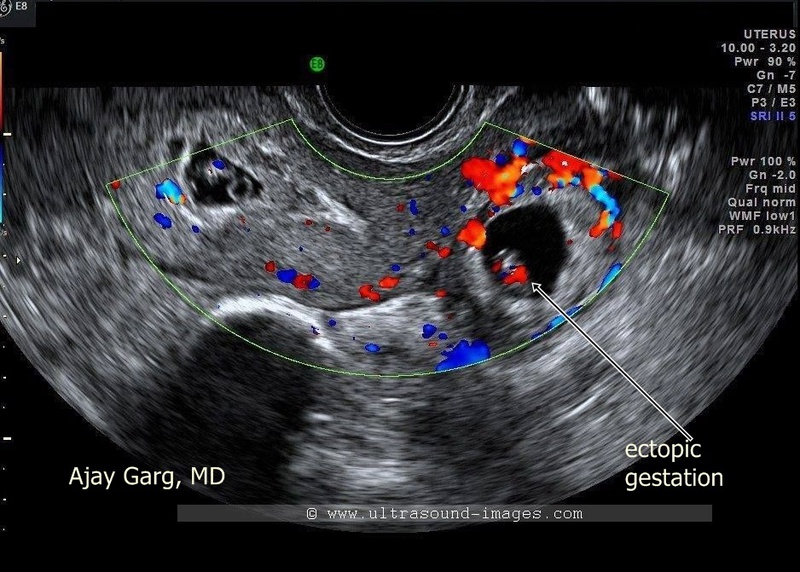
These B mode and color Doppler transvaginal ultrasound images show a classic case of heterotopic pregnancy, with an early viable embryo within an intrauterine gestation sac and another live embryo within the Fallopian tube (ectopic pregnancy) thus confirming the diagnosis. These ultrasound images by Ajay Garg, MD, prove beyond any doubt that the sac seen outside the uterus is a live ectopic pregnancy with cardiac activity visualized, meaning this is a heterotopic gestation. He used the GE- Voluson E 8 to capture these ultrasound images of heterotopic pregnancy.
Right ectopic pregnancy

Transabdominal ultrasound scan images of uterus
This patient had bleeding per vagina after testing positive for pregnancy. Ultrasound images show a sac like structure in the uterine cavity. However, the shape of the "gestation sac like structure" is elliptical with the tear drop shape suggesting something more ominous than the appearance of an anembryonic gestation. This appearance is typical of a pseudosac of ectopic pregnancy. Transvaginal ultrasound images of this case are shown below:
Transvaginal ultrasound images of uterus and adnexae



The images show a cystic mass (of 15 mm.) in the right adnexal region which is poorly vascular (this is unusual as the typical ring of fire sign of ectopic is not seen). In all probability, this is an ectopic pregnancy (right tubal gestation) which has not yet ruptured (there is little or no fluid or blood in the cul de sac). The pseudosac of ectopic gestation seen in the uterine cavity is different from the typical gestation sac in that it does not show the bright echogenic decidual reaction of a normal intrauterine gestation or even an anembryonic gestation. This patient underwent surgery for right ectopic gestation.
Another important fact: PSV (peak systolic velocity) of artery in ectopic gestation is usually > 35 cm/sac and RI > 0.7 in ectopic sac.
In corpus luteal cyst PSV is appx. = 28 cm/s
Ref: Doppler values in ectopic gestation
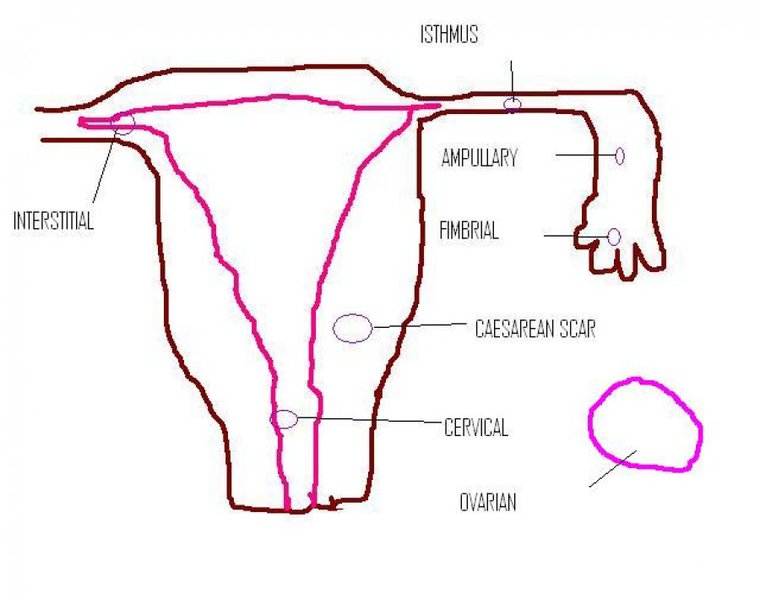
Various possible locations of ectopic pregnancy
References:
http://radiographics.rsna.org/
http://radiology.rsna.org/
Scar Pregnancy (pregnancy in LSCS scar)



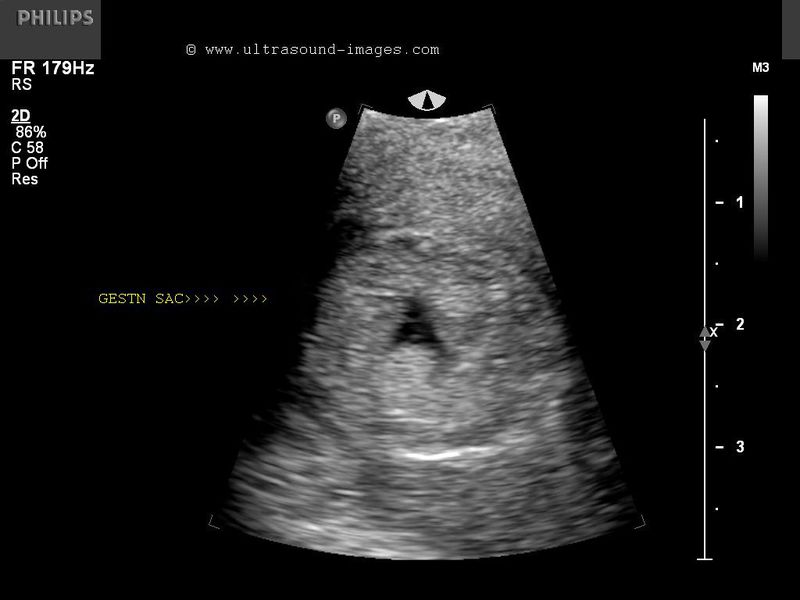
This patient presented with 5 weeks amenorrhoea and pelvic pain. She also has a history of previous caesarean section (LSCS). Ultrasound images of the uterus show a sac like structure in the lower segment of the uterus within the myometrium of the anterior wall of uterus. Color Doppler images of the uterus show increased flow (hyperemia) around the sac. Lab investigations also confirmed her pregnancy. These images suggest a LSCS scar pregnancy (caesarean scar pregnancy). Scar pregnancies are extremely rare (less than 1% of all pregnancies) and are believed to result from a canalization of the LSCS scar to the endometrial cavity. The potential for severe hemorrhage from such ectopic pregnancies is very high due to the potential for rupture of the myometrial tissue around the sac. These ultrasound images of LSCS scar pregnancy are courtesy of Dr. Nirmali Dutta, MD, Abu Dhabi, UAE.
References:
http://radiographics.rsna.org/content/28/6/1661.full.pdf+html (free excellent article and images)
http://radiology.rsna.org/content/245/2/385.full.pdf+html(free article and images)
LSCS scar Pregnancy - Case-2
Gestation sac with embryo in Cesarean scar
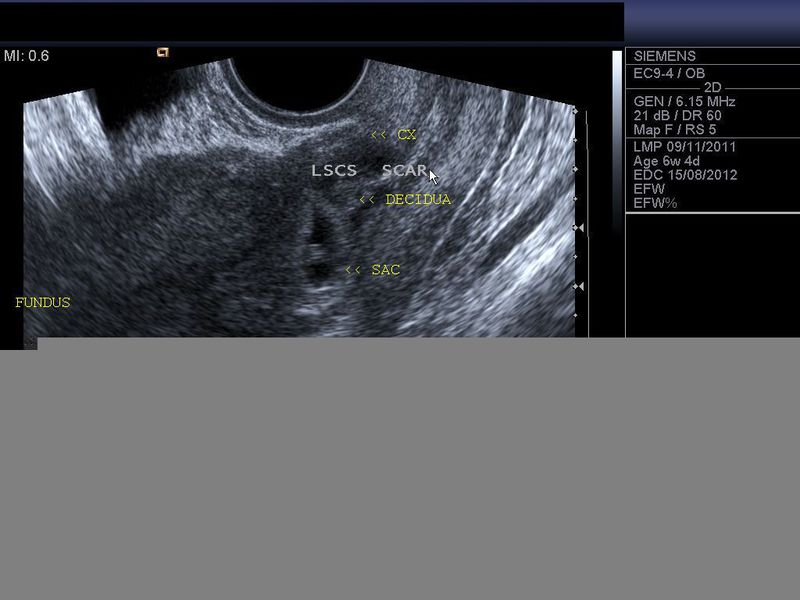


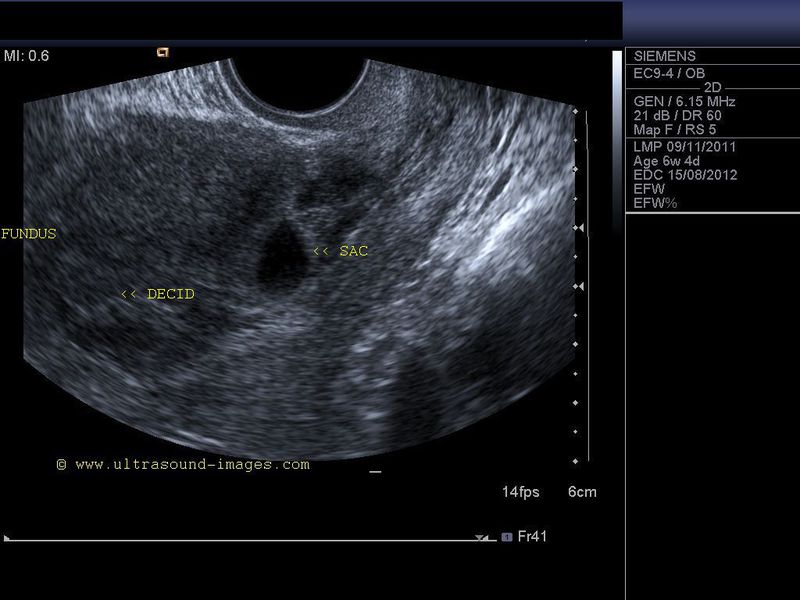
This is yet another case of Cesarean section scar pregnancy. The gestation sac with an embryo and yolk sac are seen in the lower segment. The location of the sac within the myometrium of the lower segment and with the scar tissue seen extending to the endometrial cavity are clear indicators that this is indeed a scar pregnancy. A cervical pregnancy is a close differential diagnosis; however, in cervical pregnancy the sac would lie within the endometrium and would be lower down within the cervix. The LSCS (lower segment cesarean section) scar is also visualized in these transvaginal ultrasound images ruling out a cervical pregnancy. Scar pregnancy is a type of ectopic pregnancy. Ultrasound images are courtesy of Dr. Nirmali Dutta, MD, UAE.
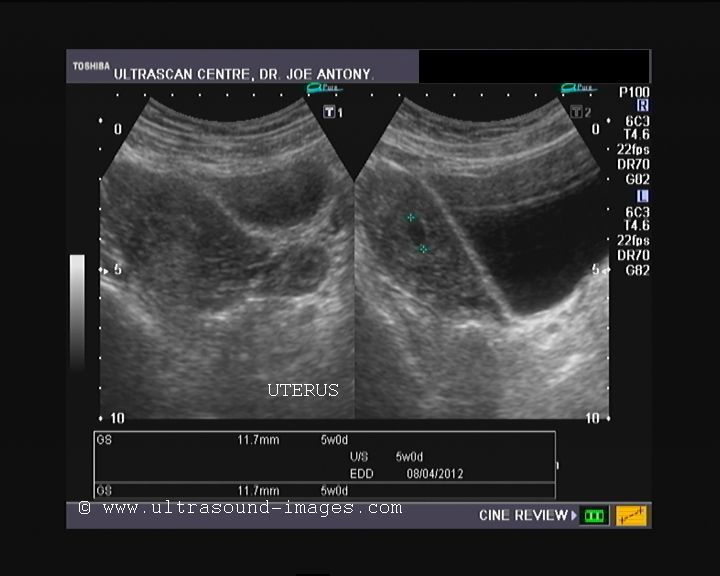
Anembryonic gestation


Sonography of early pregnancy in this case shows bulky (enlarged) gravid uterus showing a gestation sac of 13mm. (5 weeks, 1 day). The images show absence of the embryo. These ultrasound images suggest anembryonic gestation (usually known as missed abortion or blighted ovum). It is advisable to repeat the sonography (after 1 week to 10 days ), in such cases to rule out delayed development of the embryo. Other differential diagnoses include: inevitable abortion, incomplete abortion etc. One of the other causes of anembryonic gestation includes early demise of the embryo, leaving an empty sac.
Reference: http://emedicine.medscape.com/article/266228-diagnosis
Embryonic demise
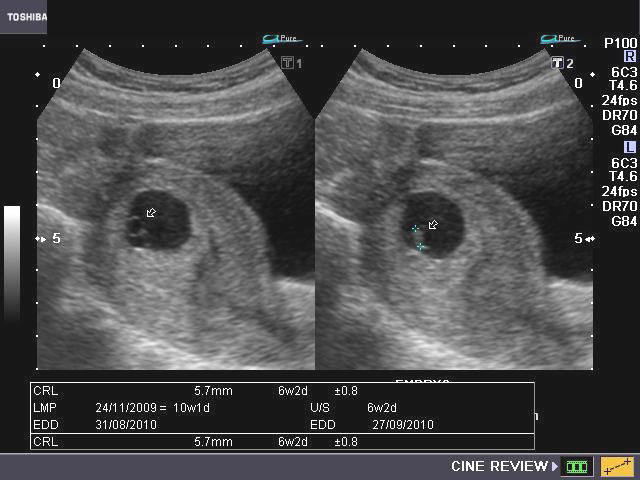
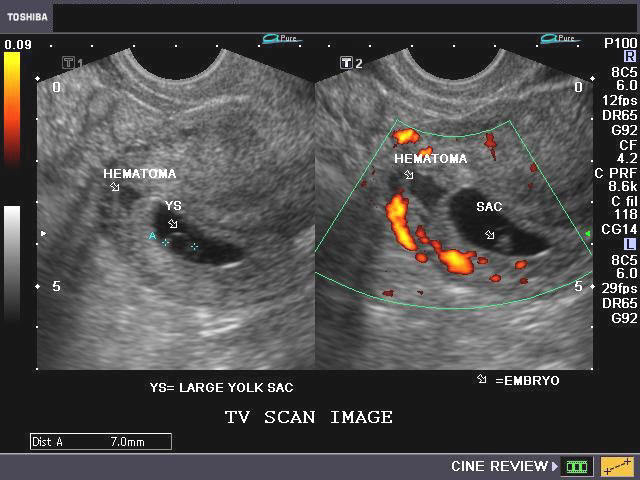
These ultrasound images show an intrauterine gestation sac with subchorionic hematoma (see transvaginal scan image in lower row), with an abnormally large yolk sac (7mm. size). This pregnancy is of 10 weeks gestational age (going by the date of last menstrual period). However the poorly developed embryo measures 6 mm. in size (6 weeks 2 days) and shows no cardiac activity which was confirmed by Power Doppler imaging. These ultrasound findings suggest embryonic demise. (Note: By current criteria, an embryo of more than 5 mm. in size showing no cardiac activity on transvaginal sonography, is considered to be non-viable/ case of embryonic demise).
Reference: http://emedicine.medscape.com/article/403208-imaging(free images and article)
Subchorionic hematoma

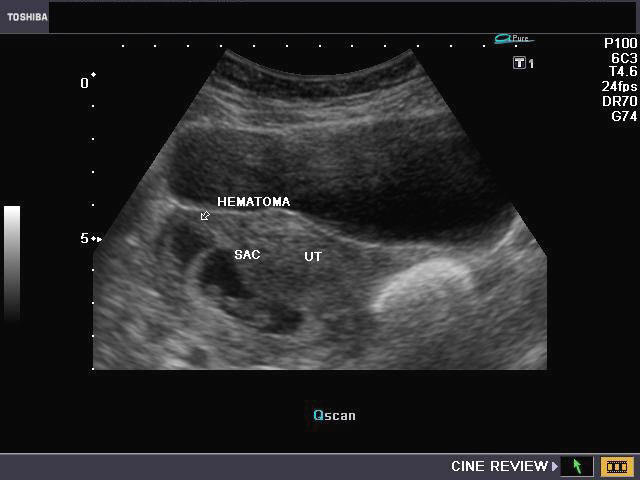
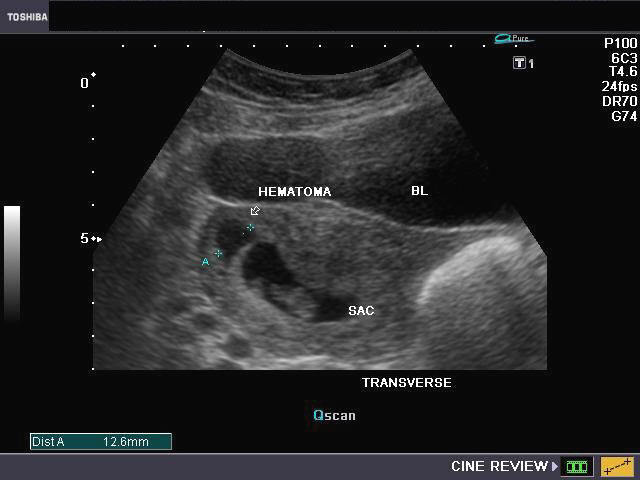
This 1st trimester patient complained of pain in the lower abdomen. Sonography of the gravid uterus shows an anechoic collection (blood--> see arrows) in the upper part of the gestation sac between the decidual tissue and the chorion. There is also evidence of separation of the margins of the earlyplacenta (abruption). The embryo, in this case, showed cardiac activity. These ultrasound images are diagnostic of subchorionic hematoma. It is advisable to follow this case with repeat sonography after 1 week and closely monitor the hematoma.
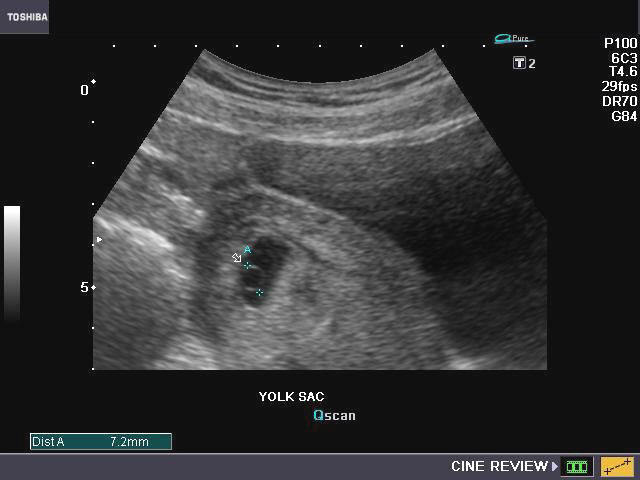
Abnormalities of yolk sac

Large yolk sac
This ultrasound image of early 1st trimester pregnancy shows a large yolk sac within the gestation sac in the uterine cavity. Both abnormally large or small yolk sacs are associated with poor prognosis and usually end in embryonic demise. No embryo was visualized in this case. A yolk sac diameter of greater than 5.6 mm. before 10 weeks gestational age indicates bad prognosis. In this case the yolk sac measured 10.6 mm. (This sonographic image is courtesy of Dr. Durr e Sabih, Pakistan).
Reference:
http://www.jultrasoundmed.org/cgi/reprint/19/9/655.pdf(free article and images)
http://radiology.rsna.org/content/183/1/115.short(free article)
Double decidual sac sign
UTERUS - SAGITTAL SECTION



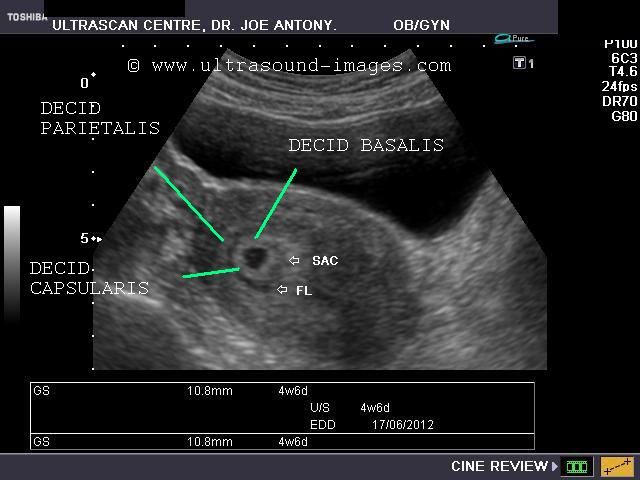
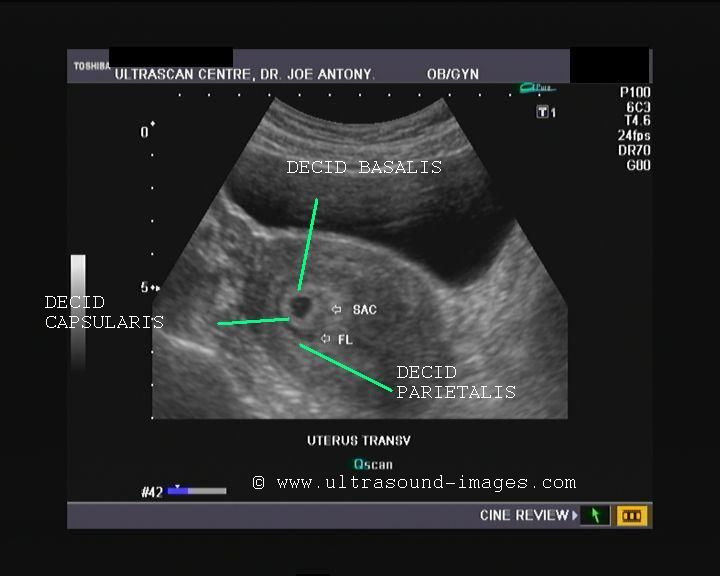
These ultrasound images show the sagittal section of the uterus in a 4 week, 6 days old pregnancy. The double decidual sac sign is clearly present, showing a normal early intrauterine pregnancy. This sign helps differentiate a normal intrauterine pregnancy in its early stages from the pseudosac of ectopic pregnancy. The double decidual sign consists of the decidua parietalis surrounding the decidua capsularis with the gestation sac encased within the Decidua capsularis. The decidua capsularis is separated from the decidua parietalis by a small amount of fluid within the endometrial cavity. The decidua parietalis lines the uterine cavity whilst the decidua capsularis encases the gesation sac. The decidua capsularis and decidua parietalis join or attached at the decidua basalis. (FL= fluid in endometrial cavity; SAC= GESTATION SAC). The double decidual sac sign is so named because of the sonographic appearance of 2 concentric rings around the gestation sac; this is a normal finding in early pregnancy.
References:
Article on double decidual sac sign (radiopedia)
Fetal ultrasound article on double decidual sac sign
3D ultrasound- early fetal demise
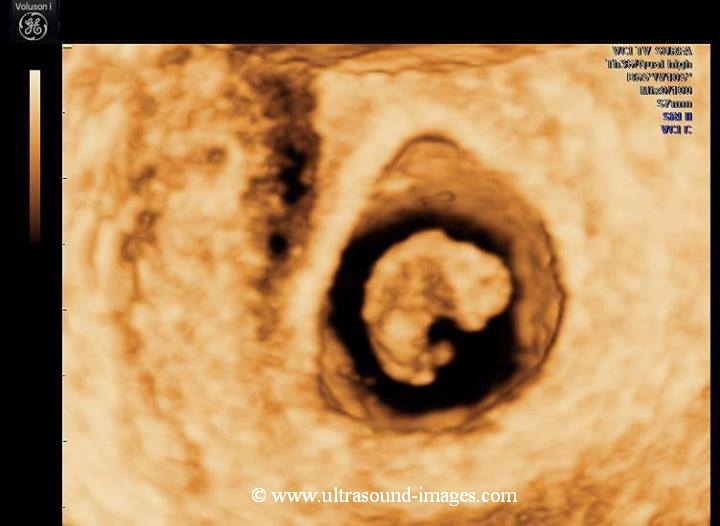
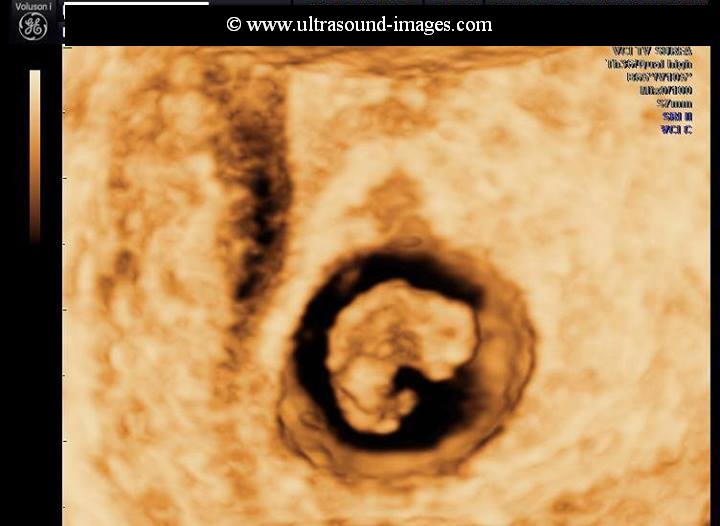
This fetus at 8 weeks shows some features on 3D-ultrasound imaging which are characteristic of fetal demise (fetal death). Observe the hyperflexed nature of the fetal body which is abnormal. In addition, the fetal limb buds are drooping, flaccidly onto the fetal body instead of normal extension outwards from the body. These findings in the above 3D ultrasound images (courtesy of Dr. Mayank Chowdhury, MD, India) are diagnostic of fetal demise.
Cervical ectopic pregnancy

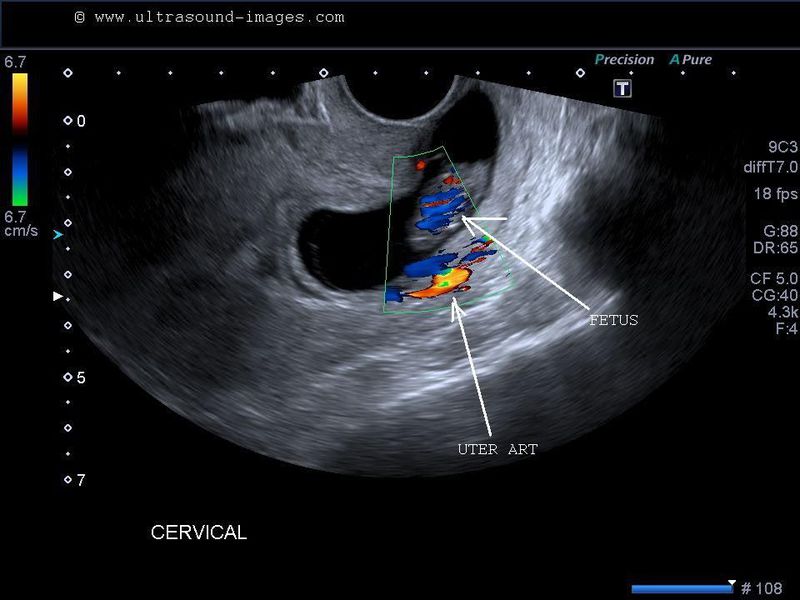

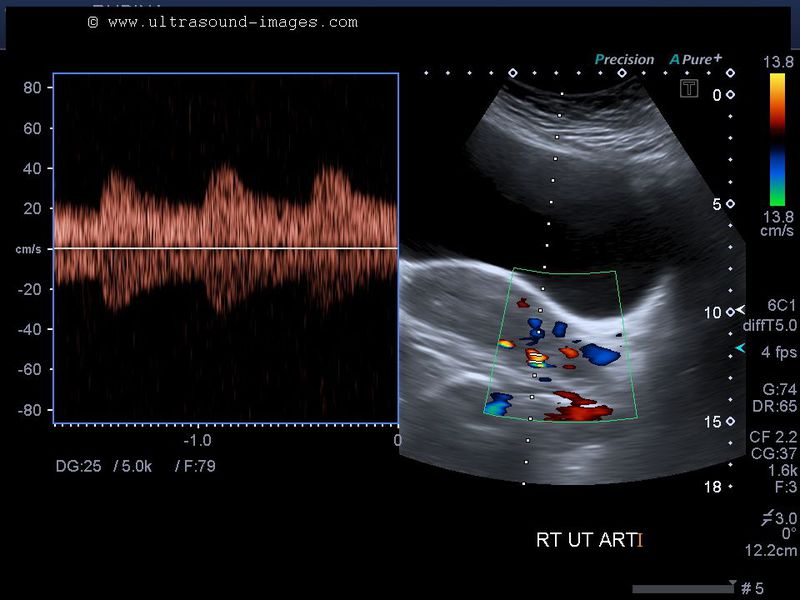
This patient had 9 weeks amenorrhoea and ultrasound imaging confirmed an intrautrerine pregnancy. However, the gestation sac of 9 weeks is located in the endocervical canal, just below the internal os. Ultrasound images shown above also show the fetus is live with color Doppler ultrasound showing cardiac activity. Thus this is an unusual gestation- a live cervical ectopic pregnancy. The presence of fetal cardiac activity is diagnostic of a cervical ectopic pregnancy as seen in these ultrasound images. The main differential diagnosis is an abortion in progess, in which case the fetus would not show cardiac activity due to fetal demise. The uterine artery is also seen in these images with the gestation sac below the level of the uterine artery. These images of cervical ectopic gestation are courtesy of Dr. Durr-e-Sabih, FRCP.
Abdominal ectopic pregnancy
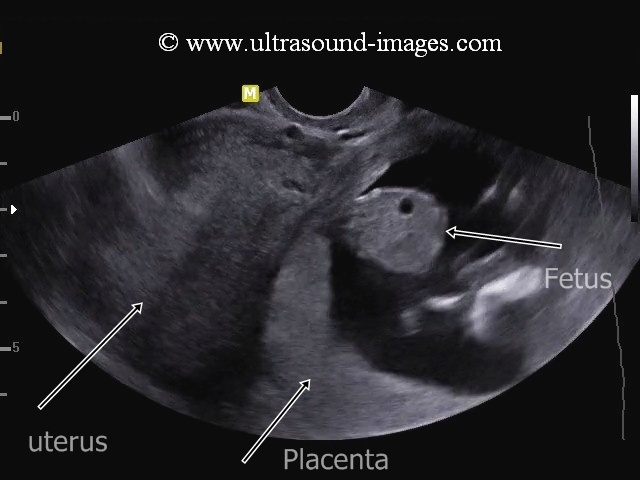
This lady underwent ultrasound imaging during early pregnancy, which showed absence of an intrauterine pregnancy, but showed a left adnexal mass lesion ( left tubal ectopic pregnancy). However, the patient opted not to undergo any surgical treatment and was put on tocolytics. The patient wished to have a second opinion after a few weeks. On the second ultrasound examination, a 16 weeks old fetus was visualized outside the uterine cavity in the left hemi-pelvis. The following points helped arrive at a diagnosis of the left pelvic, abdominal ectopic pregnancy:
1. At 16 weeks old, live fetus with posterior placenta was seen outside the uterine cavity. There was no evidence of myometrial tissue between the pregnancy sac and fetus and the urinary bladder.
2. The history of a left adnexal mass, which in all probability was a tubal ectopic pregnancy; which subsequently ruptured resulting in left abdominal ectopic pregnancy. These findings were confirmed on surgery.
The presence of a live and relativlely large fetus outside the confines of the uterine cavity is almost certainly, a sign of an abdominal ectopic pregnancy. These ultrasound images of abdominal ectopic pregnancy are courtesy of Dr. Darshna Pandya, MD. an abdominal ectopic pregnancy can usually occur following rupture of a tubal gestation with subsequent implantation within the pelvis, along the omentum, great vessels, or other pelvic structures, including intestines. The danger of complications like severe haemorrhage make an abdominal ectopic pregnancy a surgical emergency.
References: Ultrasound imaging of abdominal ectopic pregnancy
Live-ectopic-pregnancy

This 6 weeks embryo is seen in left Fallopian tube, and showed cardiac activity or pulsations- a live tubal ectopic pregnancy, a comparatively rare event. In this case the patient had no symptoms to suggest an ectopic pregnancy, neither pain nor tenderness or abnormal bleeding p/v. After the ultrasound scan, per vaginal examination showed left fornical tenderness. On ultrasound the uterus showed absence of gestation sac- one of the possibilities being a complete abortion. However, minimum fluid was present in the cul de sac- a warning sign of tubal ectopic pregnancy. On transvaginal ultrasound scan the left adnexa showed a vascular ring shaped lesion next to the left ovary, and contained a live embryo with cardiac activity- a clear sign of live ectopic pregnancy. This patient underwent surgery and the diagnosis was confirmed.
live-ectopic-12weeks-case-2

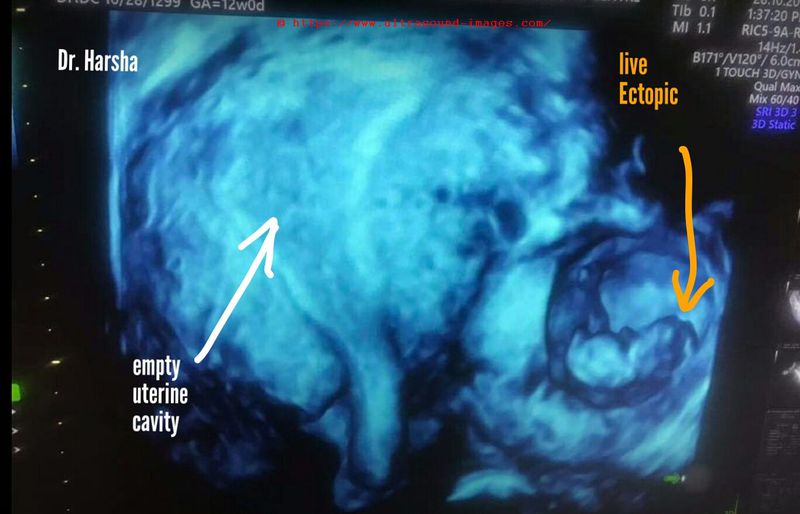
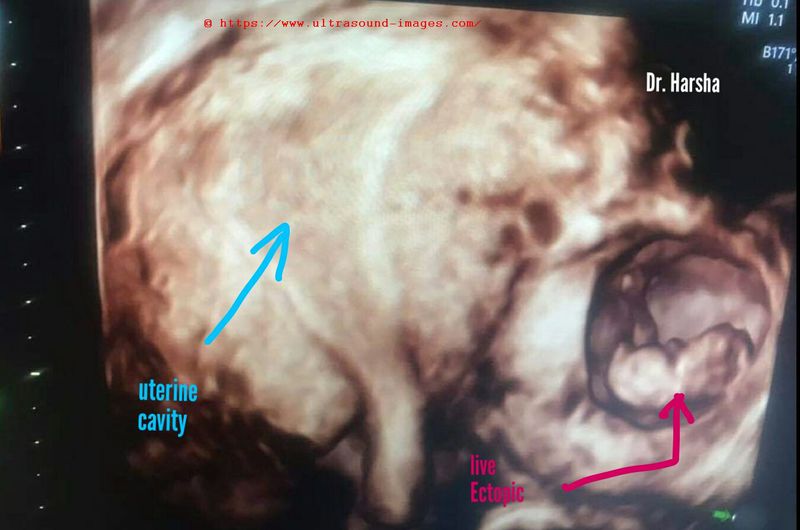
This 12 week fetus seen in left adnexal region appears to be a tubal or ovarian live ectopic pregnancy. 2D B-mode and 3D/ 4D ultrasound Images courtesy of Dr. Harsha Juneja Sehgal, MD, DGO, India.This fetus showed cardiac activity and fetal movements.
low-implantation-gestation-sac
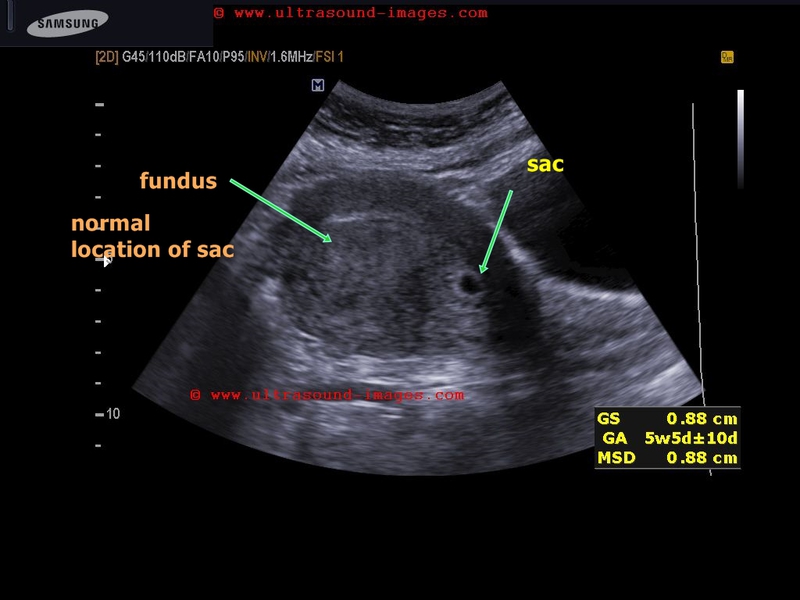
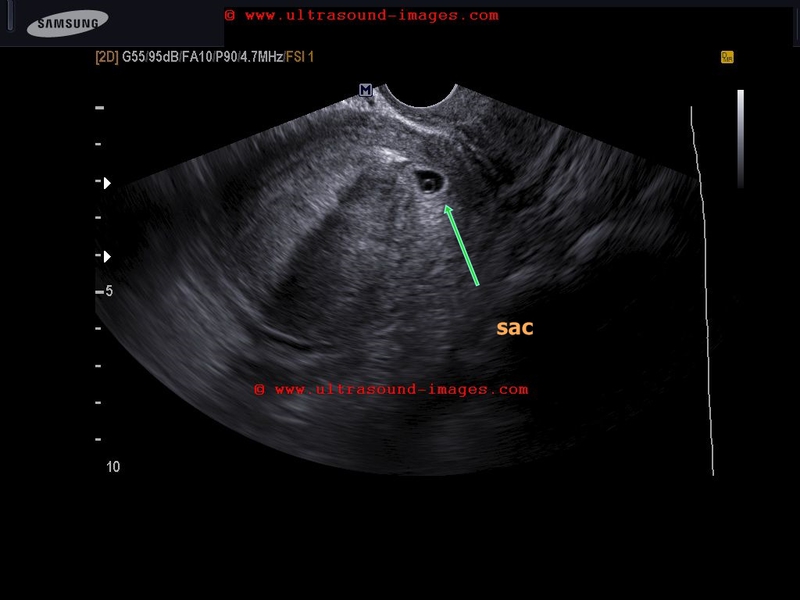
In this patient, the gestation sac is located in the lower uterine segment just above the cervix. This suggests low implantation of gestation sac. Yolk is present within the sac.
The prognosis for such cases is poor due to the threat of imminent abortion.
Follow up is needed to assess progress of this case.
References: low implantation of sac
© 2026, Joe Antony, MD All images and content in this site are copyrighted. www.ultrasound-images.com When visiting this site, we may use cookies to improve the performance of this site. Use of this site means you accept the use of cookies. Read our privacy policy at this page: https://www.ultrasound-images.com/privacy-policy/