
Pediatric
Contents of this page
- Inguinal hernia in neonate containing ovary
- Another case of inguinal hernia with ovary in infant
- Intraventricular adhesions- in the lateral ventricles
- Pulmonary consolidation with pleural effusion
- Intracranial hemorrhage
- Complications of intraparenchymal hemorrhage- porencephalic cyst of brain
- Another complication of subependymal hemorrhage- subependymal cysts
- Hydrocephalus
- Another case of Hydrocephalus in neonate
- Basal ganglia calcification in neonate with Down syndrome
- Sacral meningocele in neonate
- Sacral myelomeningocele in neonate
- AGENESIS OF THE CORPUS CALLOSUM in AICARDI SYNDROME
- Lobar Holoprosencephaly with partial agenesis of corpus callosum
- Periventricular leukomalacia in neonate
- Cerebral edema in neonate
- Vein of Galen malformation in neonate (synonym: vein of Galen aneurysm)
- Intraspinal cystic lesion in lumbo-sacral region -of neonate (filar cyst vs. ventriculus terminalis)
- meningitis-neonate
- intraventricular-debris-ventriculitis
- absent-septum-pellucidum
Inguinal hernia in neonate containing ovary

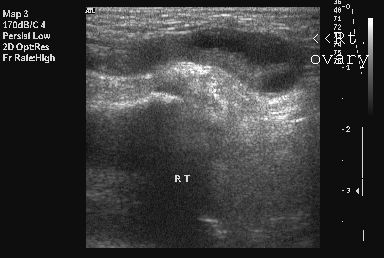
This 6 week old female child had a swelling in the right inguinal region. Ultrasound images reveal a hypoechoic elongated mass (the processus vaginalis) with an oval structure showing cystic areas. This suggests a right inguinal hernia containing the right ovary. Such hernias usually do not resolve spontaneously. Images courtesy of Dr. Nirmali Dutta, UAE. Ultrasound machine used is the Philips HDI 5000.
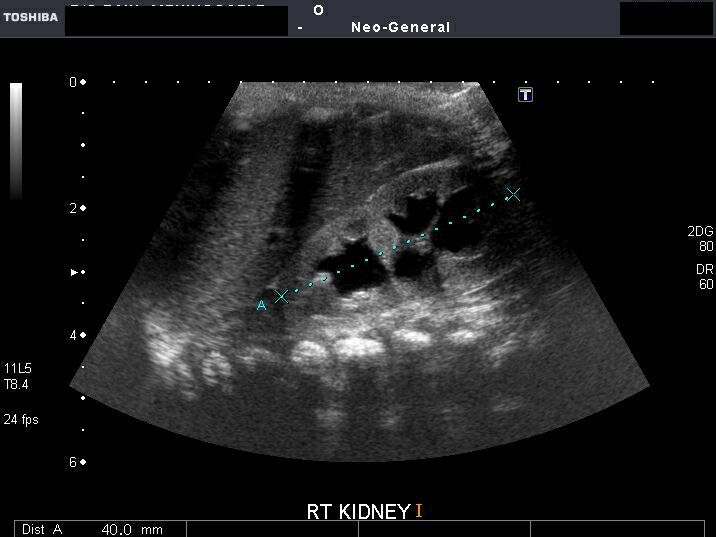
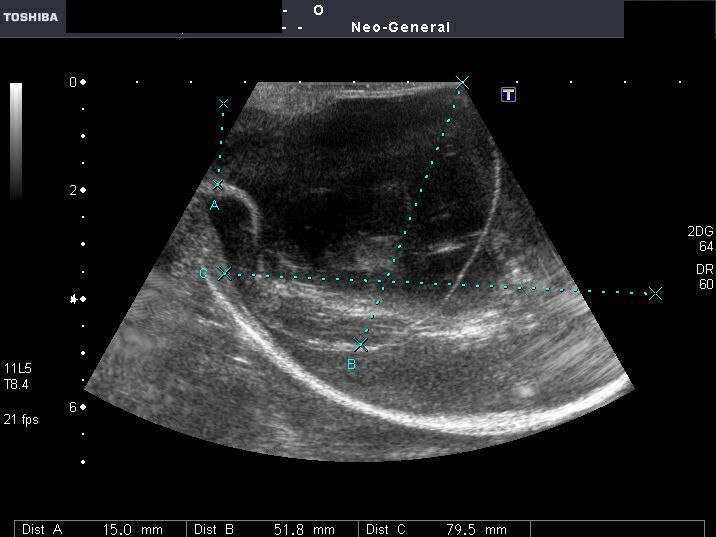
Another case of inguinal hernia with ovary in infant
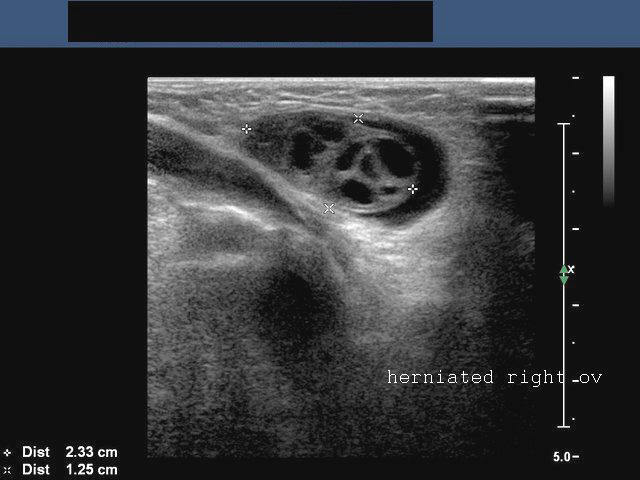
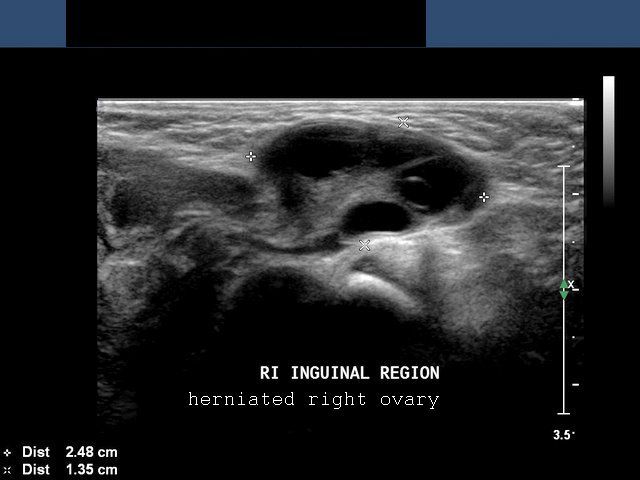
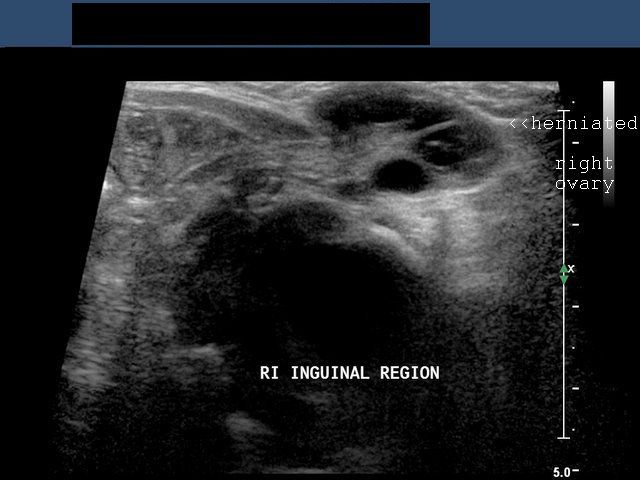
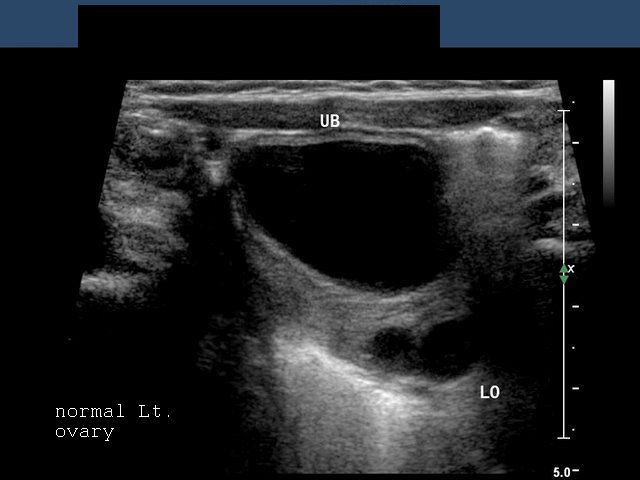
The above ultrasound images show a female neonate with right inguinal hernia containing the right ovary. The right ovary is seen as an oval structure with multiple small cystic areas (follicles). The defect in the abdominal wall is also visualized in these ultrasound images. The image on bottom right shows the normal left ovary located posterior to the urinary bladder. These ultrasound images are courtesy of Dr. Ravi Kadasne, UAE.
Reference:http://www.jultrasoundmed.org/cgi/reprint/26/7/985.pdf
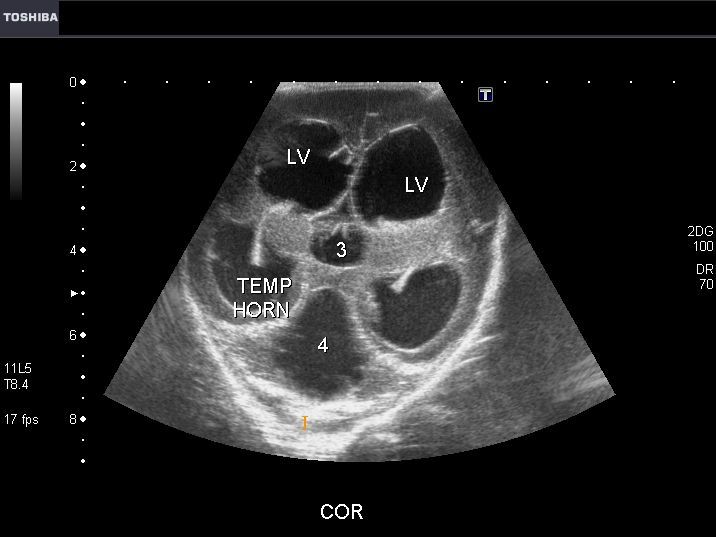
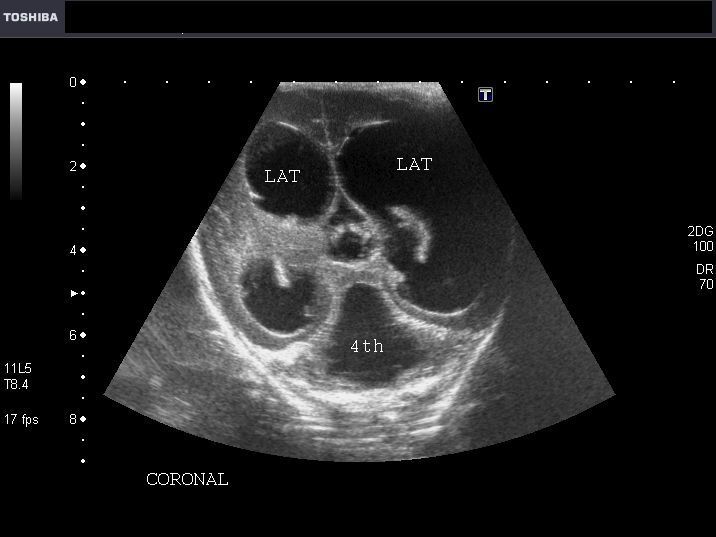
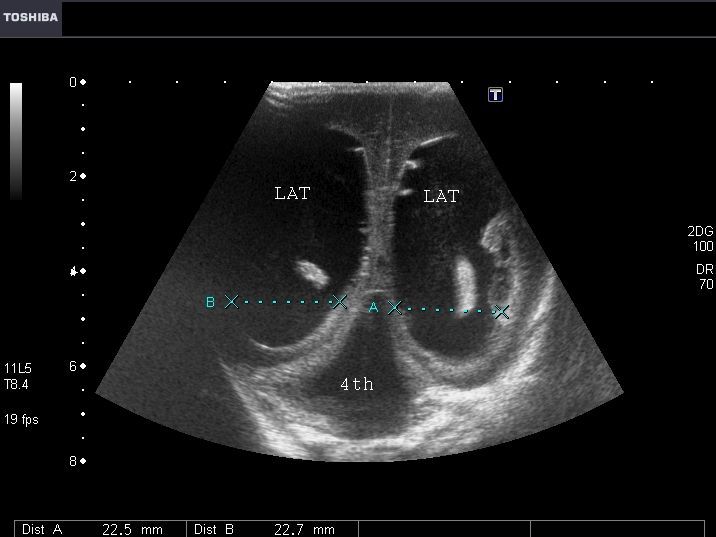
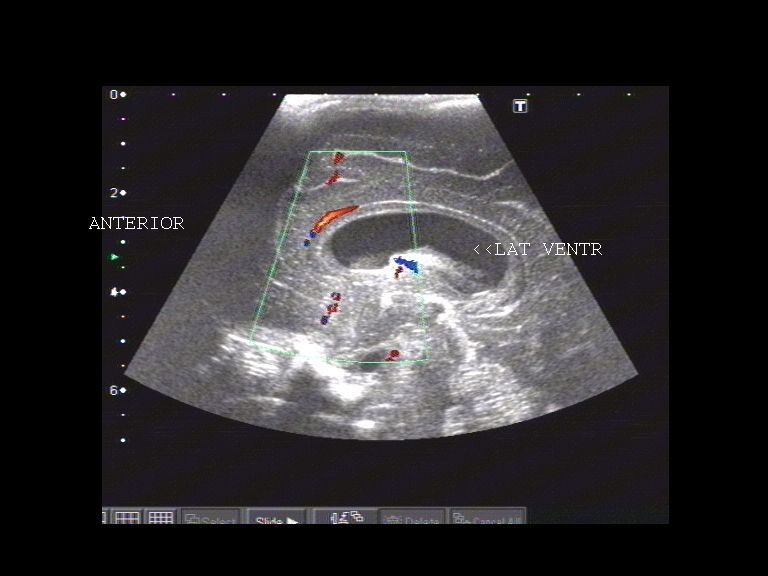
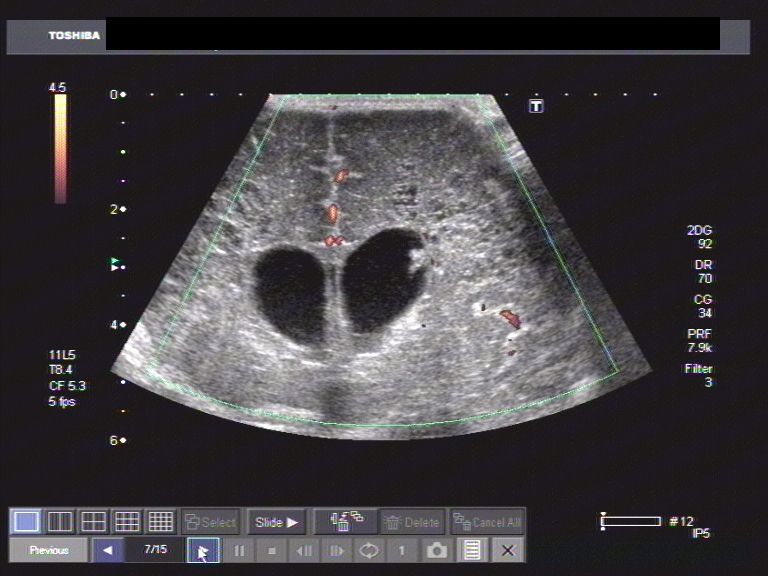
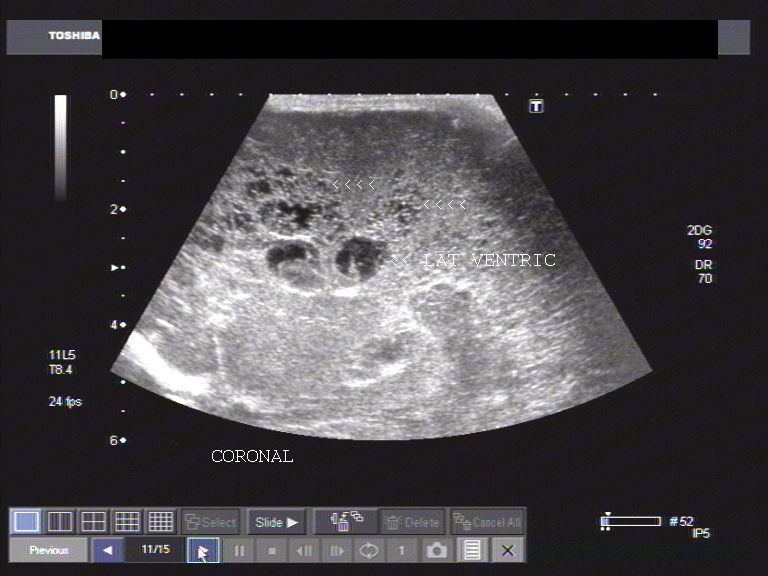
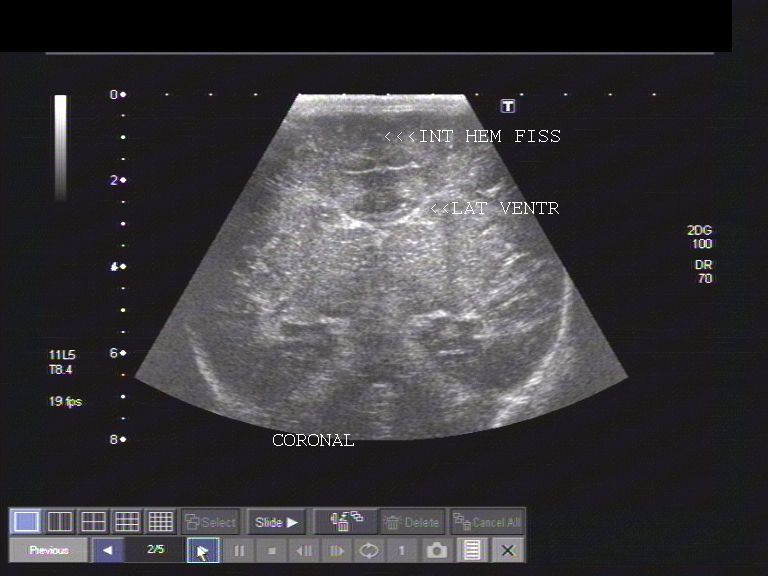
Intraventricular adhesions- in the lateral ventricles
My e-book for Amazon Kindle- Atlas of neonatal ultrasound is
available at:
Atlas of neonatal ultrasound- cranium and abdomen
for other countries:
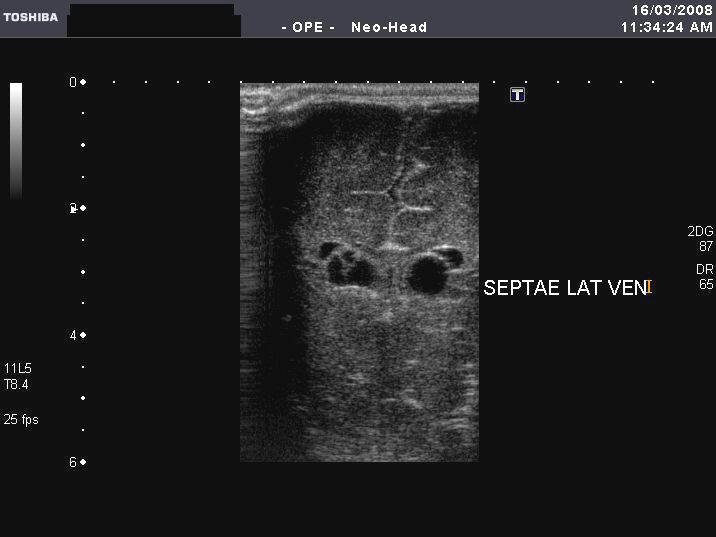
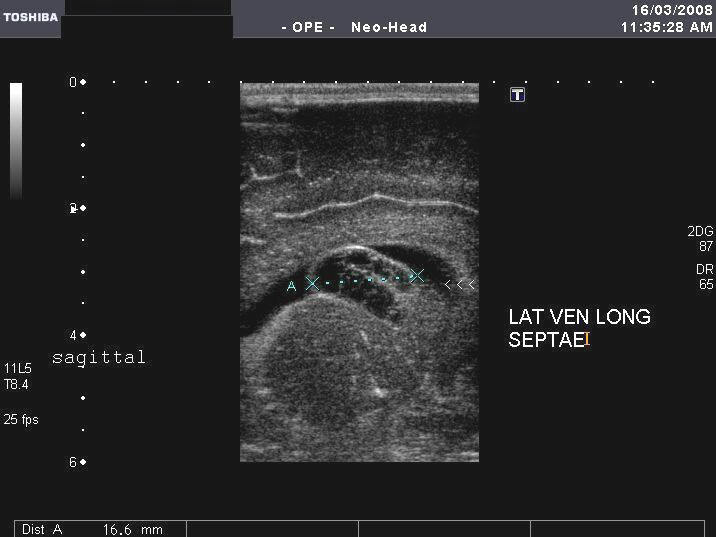



Sonography of the brain in this neonate reveal multiple septae or adhesions within the lateral ventricles. There is no evidence of hydrocephalus or intracranial hematoma. These ultrasound images suggest some form of ventriculitis, causes of which include 1) old intraventricular hemorrhage 2) any form of encephalitis (eg: cytomegalovirus infections). Ultrasound images taken by Dr. Joe Antony, using a Toshiba Xario ultrasound machine.
Pulmonary consolidation with pleural effusion
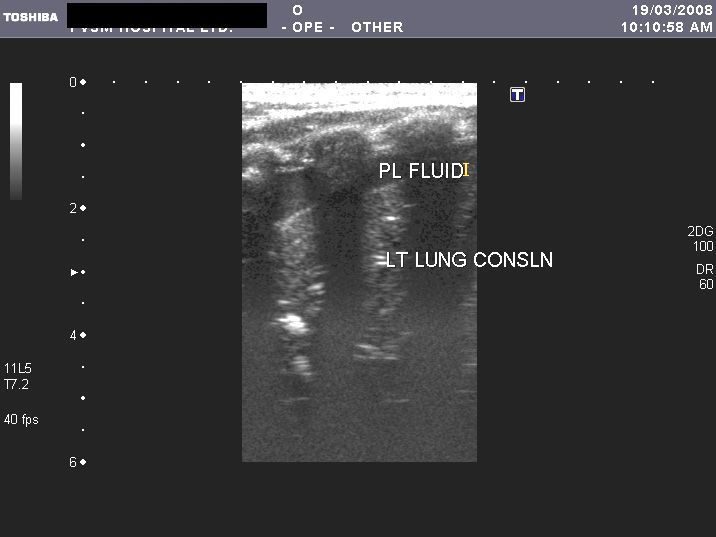


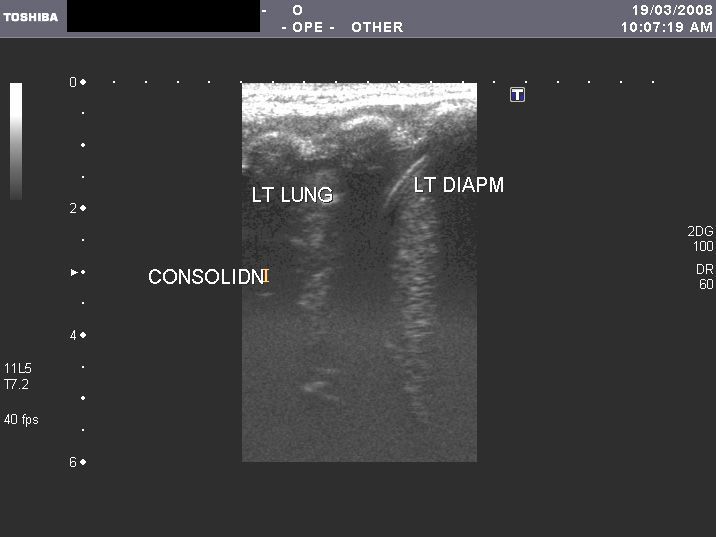
This young child shows an anechoic collection (of fluid) in the left pleural cavity. The left lung (lower lobe) shows echogenicity and texture similar to that of the liver (hepatisation). The spleen is seen below the left hemidiaphragm. These ultrasound images suggest left pulmonary consolidation with left pleural effusion. Images taken using a Toshiba Xario ultrasound machine, by Dr. Joe Antony, Cochin.
Reference: http://www.jultrasoundmed.org/cgi/content/full/26/7/985 (an excellent free article with images).
Intracranial hemorrhage
(Germinal matrix hemorrhage/ Hypoxic-ischemic events in neonates)
a) Germinal matrix hemorrhage-Grade-1: Subependymal hemorrhage


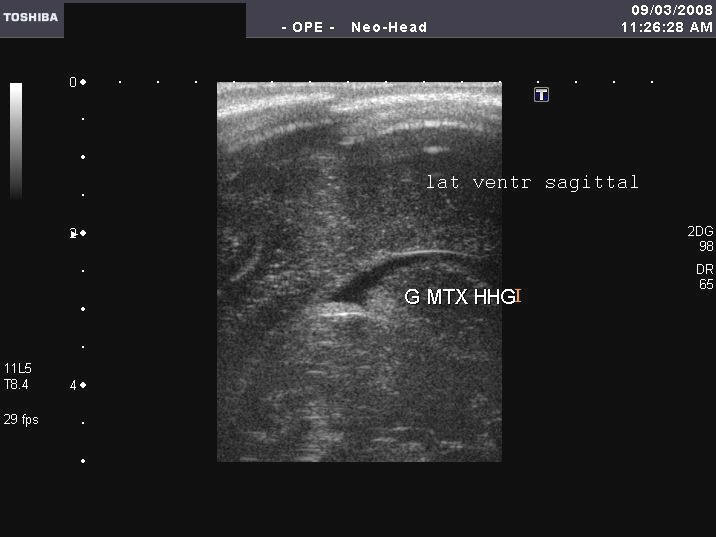

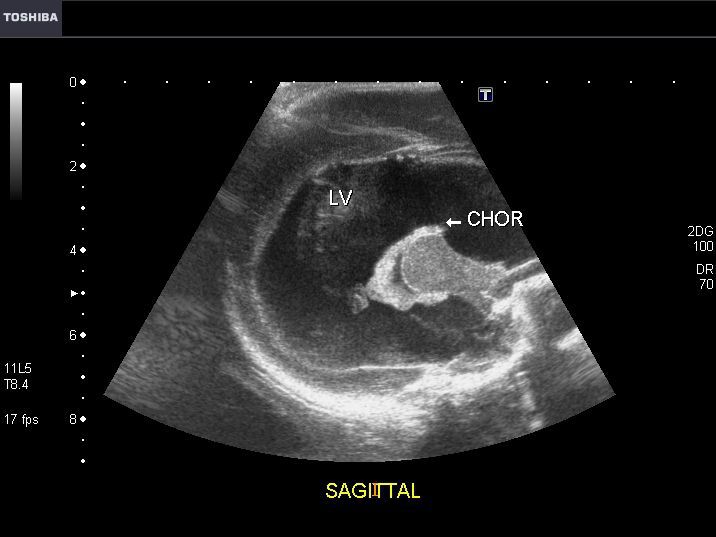
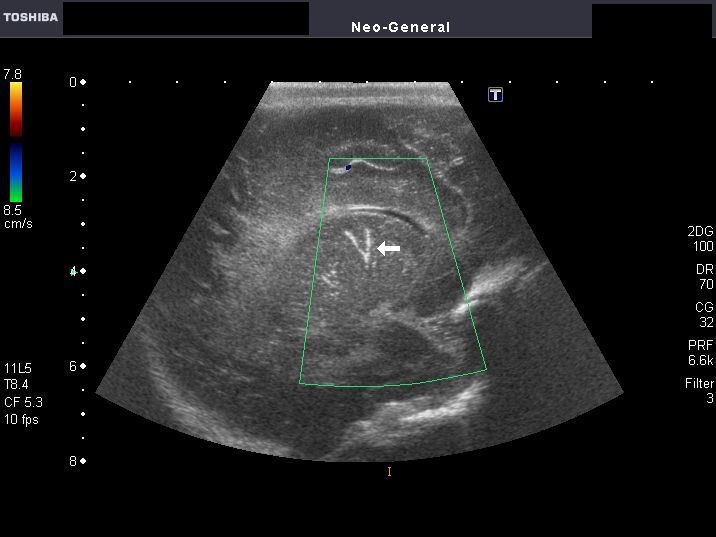
These sonographic images of neonatal brain show echogenic material in the caudothalamic groove, the region of the germinal matrix. These ultrasound images suggest grade-1 germinal matrix hemorrhage. The ventricles are of normal size and show minimal intraventricular hemorrhage (IVH). Images taken by Dr. Joe Antony, using a Toshiba Xario machine.
One of the first signs of IVH or intraventricular hemorrhage is a bulky irregular choroid plexus- this is because of hemorrhagic matter alongside the choroid plexus.
If choroid is larger or bulky on one side, this is highly s/o IVH.
Also the presence of blood within the frontal horns of lateral ventricles - seen as echogenic matter.
see: bulky choroid plexus as a sign of IVH
b) Germinal matrix hemorrhage- Grade-3



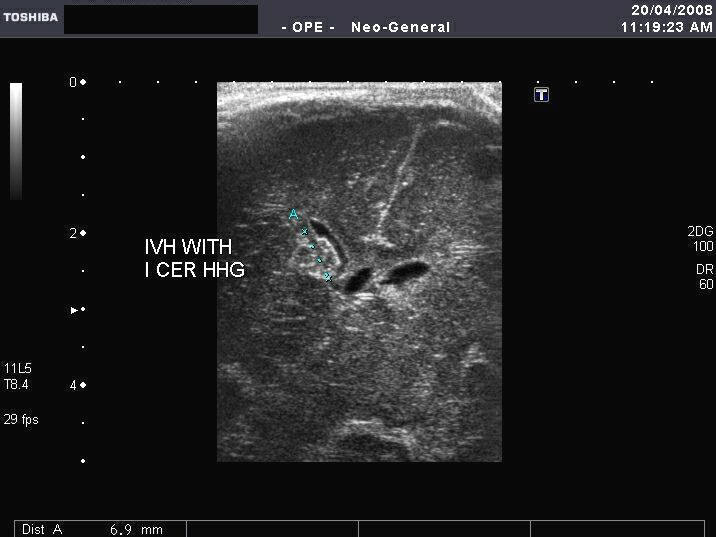
Ultrasound images of this neonatal brain shows massive IVH (intraventricular hemorrhage) from the germinal matrix. The IVH (bleed) is seen as intensely hyperechoic material exteding into both lateral ventricles from the frontal to the occipital horns. The choroid plexus is obscured by the IVH. There is no significant intracerebral extension of the hematoma. However, early hydrocephalus is present. This suggests grade-3 germinal matrix hemorrhage in this neonate. Germinal matrix hemorrhage is graded from 1 to 4 as follows:
GRADE-1: There is subependymal hemorrhage
GRADE-2: There is IVH without hydrocephalus
GRADE-3: There is IVH with hydrocephalus
GRADE-4: There is IVH with intraparenchymal hemorrhage. (Hydrocephalus may or may not be present).
c)Germinal matrix hemorrhage- Grade 4



The above 3 ultrasound images (Toshiba Xario machine) show- grade 4 germinal matrix hemorrhage- subependymal bleed with intraventricular hemorrhage (IVH) and intraparenchymal extension. There is also a small subependymal cyst.
Follow -up scan 1 week later
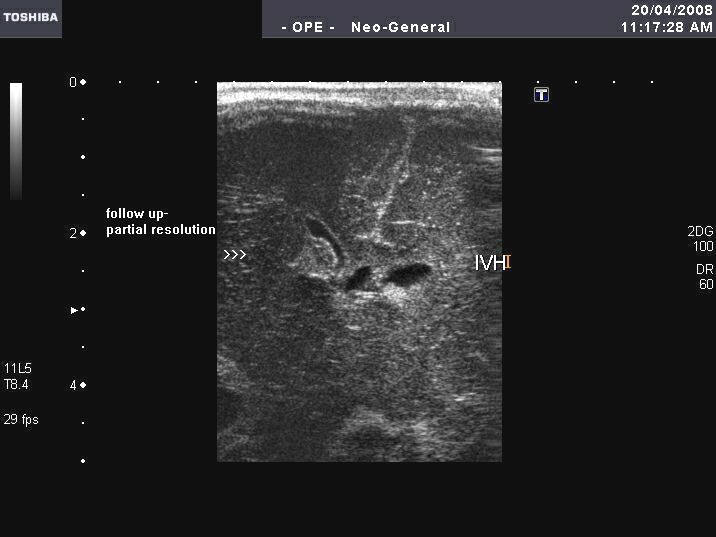

Follow up ultrasound scan (1 week later) show partial resolution of the hematoma and the IVH.
Large intracerebral hematoma in neonate

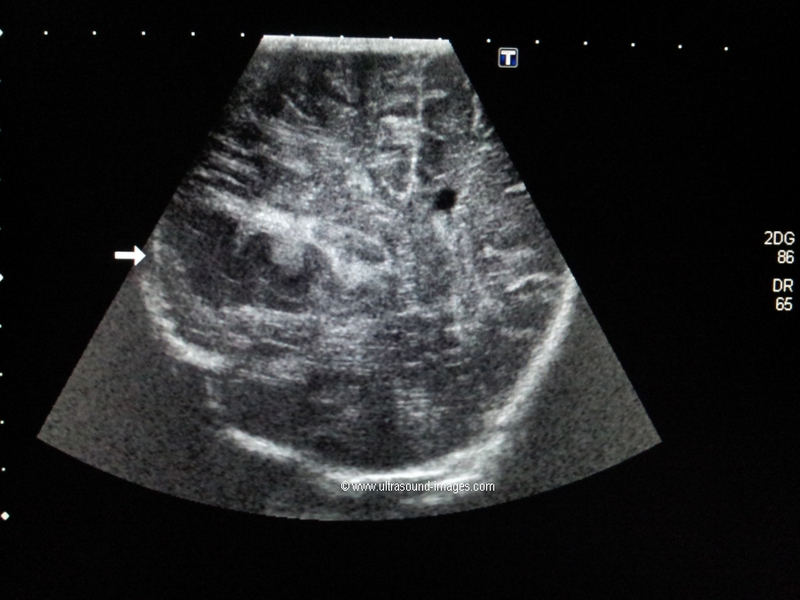
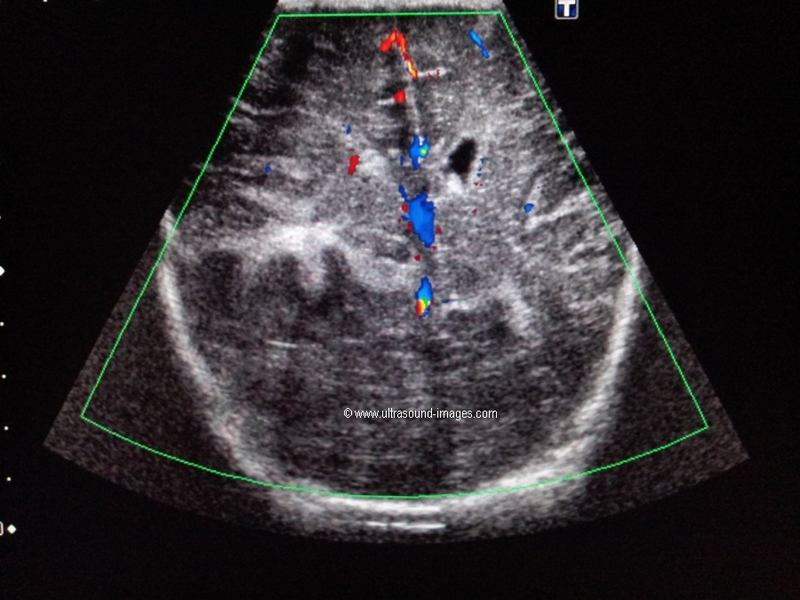


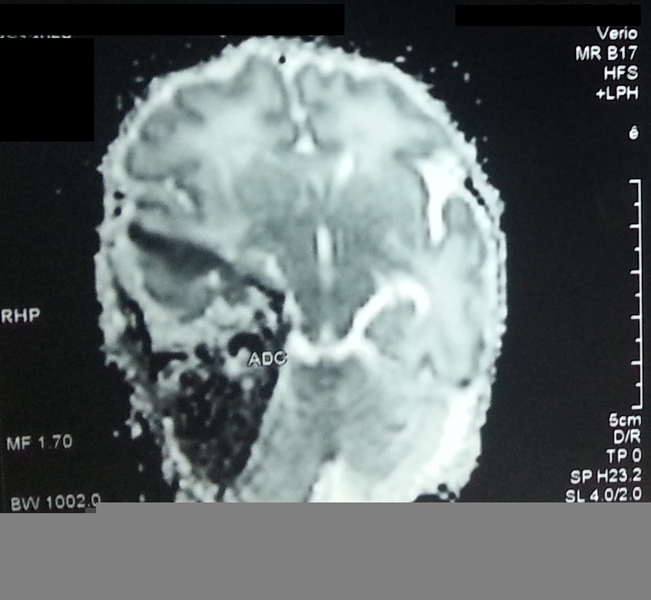

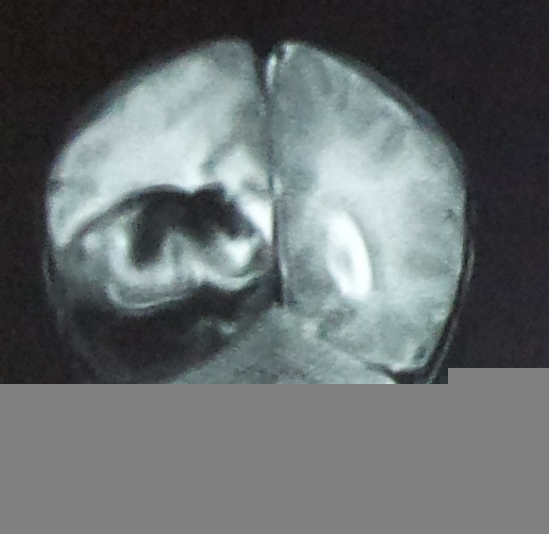
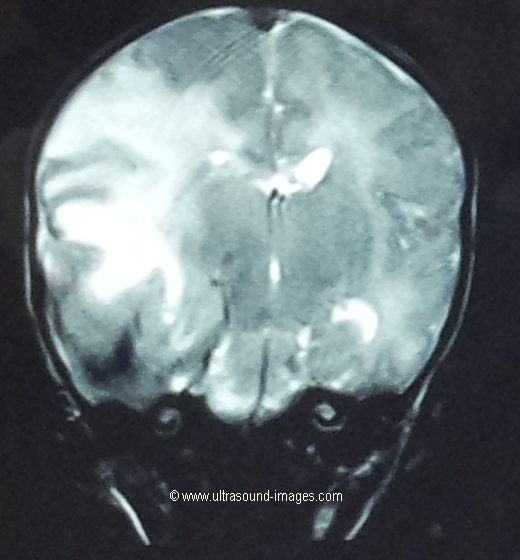
This neonate has a very large intracerebral hematoma in the right parieto-occipital region of the brain, producing a significant mass effect with midline shift to the left. There's effacement of the right lateral ventricle also.
The initial appearances on ultrasound suggested a possible heterotopia. However, MRI scan suggests a large subacute intra cerebral haematoma in this region. There is also significant oedema within the cerebral tissue.
Another possible differential diagnosis in this neonate is an intracranial space occupying lesion such as a glioma. However, this diagnosis can be excluded based on the MRI findings. On ultrasonography, it may often be difficult to come to a precise diagnosis of such large space occupying lesions in the neonatal brain.
This link on heterotopia can be useful reading:
http://www.ajnr.org/content/30/1/4.full
Complications of intraparenchymal hemorrhage- porencephalic cyst of brain

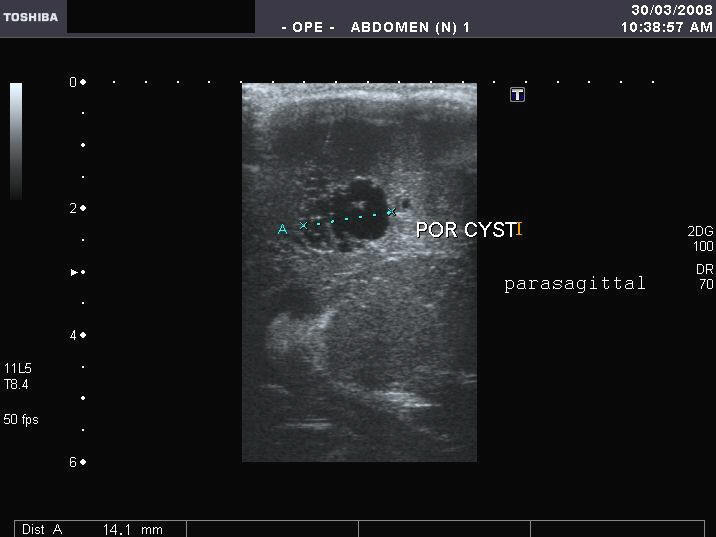


Sonography of the brain in this neonate shows a cystic lesion in the periventricular region of the cerebral hemisphere. Measuring 10 x 14 mm., it appears thin walled and may have a communication with the lateral ventricle. These ultrasound images are highly suggestive of a porencephalic cyst of the brain. These are formed after resolution of a hematoma originating from the germinal matrix, with parenchymal extension. The lowermost image shows an associated subependymal cyst.
Reference: http://www.ajronline.org/cgi/reprint/138/3/467.pdf(free- excellent article and images).
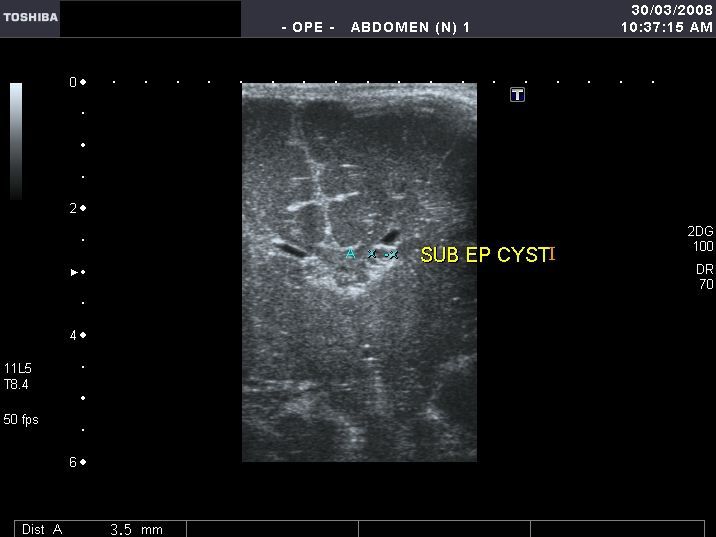
Another complication of subependymal hemorrhage- subependymal cysts


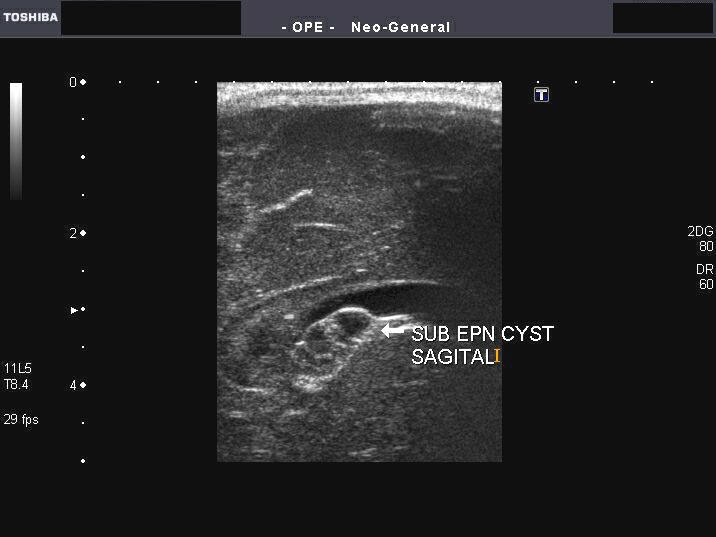
Sonography of the neonatal brain reveals a large subpendymal cyst of 3.5 mm. in the left caudato-thalamic groove. Sagittal section image also shows the true extent of the cyst. Such subpendymal cysts are a known complication of subependymal hemorrhage in neonates. Other causes of such cysts are intracranial infections. These are known to resolve spontaneously. The right side shows evidence of subependymal hemorrhage.
Reference: http://www.ajronline.org/cgi/reprint/162/4/953
Hydrocephalus


In this neonate, there is evidence of considerable enlargement of the lateral ventricles. Measurement at the atria are more than 12 mm. on both sides. These ultrasound images suggest hydrocephalus. Images taken by Joe Antony, MD, using a Toshiba Xario ultrasound machine.
Another case of Hydrocephalus in neonate
Sonography of this neonatal brain shows severe dilatation of both lateral ventricles, the 3rd ventricle and also the fourth ventricle. The lateral ventricles measure 2.3 cms. at the atria. There is evidence of thinning of the cerebral tissue. The echogenic choroid plexus is seen within the lateral ventricles, near the thalami. There was no evidence of spinal dysraphism or extra- CNS anomalies. These ultrasound images are suggestive of communicating or extraventricular obstructive hydrocephalus. Here, the site of obstruction appears to be outside the ventricular system or failure of absorption of the CSF.
Reference: http://emedicine.medscape.com/article/1135286-overview(free article).
Basal ganglia calcification in neonate with Down syndrome



This male neonate showed evidence of Down's syndrome. Sonography of the brain showed linear calcific lesions in the basal ganglia, bilaterally. Color doppler imaging showed the linear echoes not to be of vascular nature. Such linear calcific lesions are known to occur in Down's syndrome, as well as other common conditions as prematurity, cerebral anoxia and intrauterine infections. Upper 2 ultrasound images show coronal section through the brain. Lower 2 ultrasound images show linear calcification in sagittal section. All images were taken by Joe Antony, MD, using a Toshiba Xario ultrasound machine.
References:
1)http://journals.elsevierhealth.com/periodicals/ymai/medline/record/MDLN.157246
2) http://www.ncbi.nlm.nih.gov/pubmed/7094616
Sacral meningocele in neonate



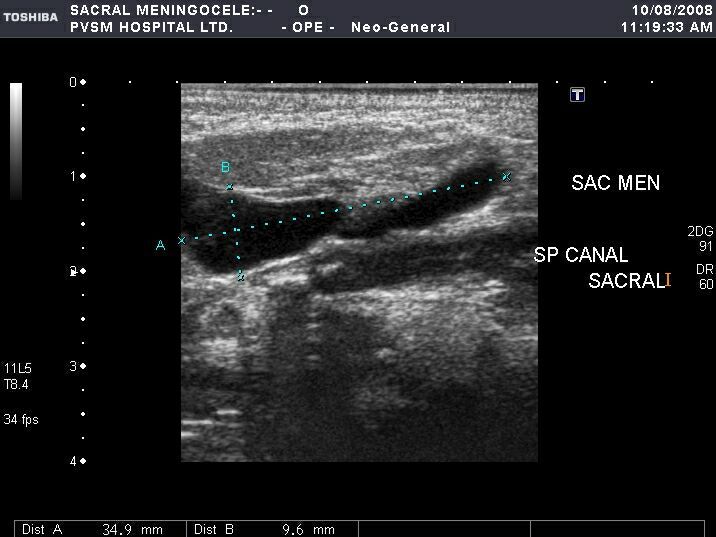

This neonate had a small swelling on the dorsum of the sacral region. Sonography of the swelling revealed: 1) a sac measuring 1.0 x 3.2 cms. posterior to the sacrum, containing clear fluid (CSF), 2) communicating with the spinal canal through a defect (spinal dysraphism), measuring 1.1 cms. 3) low tethering of the spinal cord. These ultrasound images of the neonatal spine are diagnostic of sacrococcygeal meningocele. Note that the sac does not contain neural tissue. Images taken by Dr. Joe Antony, MD, using a Toshiba Xario machine.
Reference:http://bjr.birjournals.org/cgi/content/full/75/892/384(free article and images) .. excellent
Sacral myelomeningocele in neonate

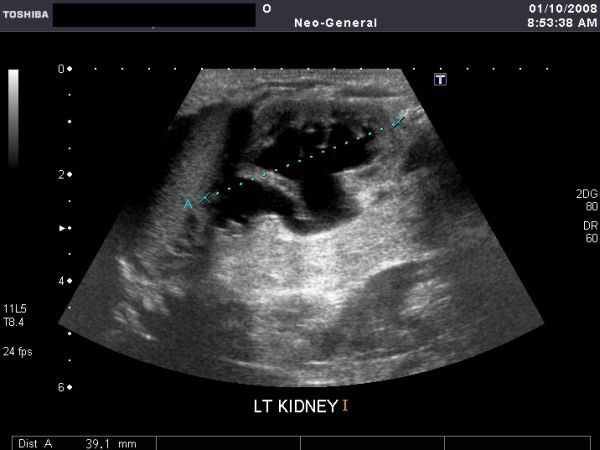


This neonate showed a large sac on the dorsal aspect of the sacrum, extending to the coccyx. Sonography of the sac revealed a large fluid filled mass with a sac like structure (sac) within the main sac. A defect is seen in the sacral vertebrae. The inner sac measures 5.2 cms. approximately while the outer one measures 8 cms. The defect is 1.5 cms. in width. These ultrasound images favor a diagnosis of sacral myelomeingocele (with the inner sac being the herniated, expanded spinal cord). The neonatal brain showed normal ultrasound appearance whilst the kidneys appeared hydronephrotic (possibly due to a neurogenic urinary bladder, a consequence of the myelomeningocele). Images by Joe Antony, MD using a Toshiba Xario ultrasound machine.
Reference:http://bjr.birjournals.org/cgi/content/full/75/892/384 (free article and images) .. excellent
AGENESIS OF THE CORPUS CALLOSUM in AICARDI SYNDROME
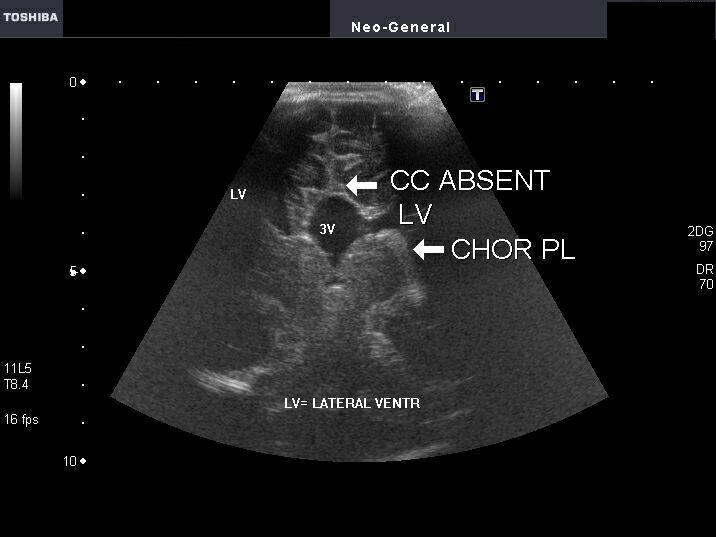

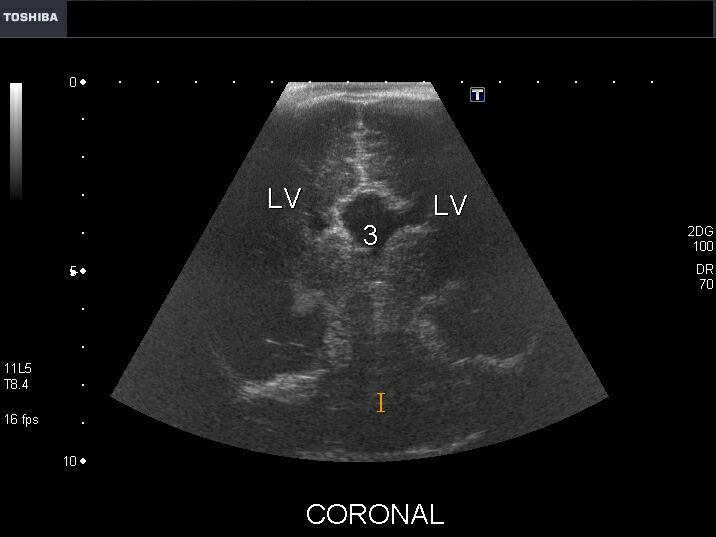
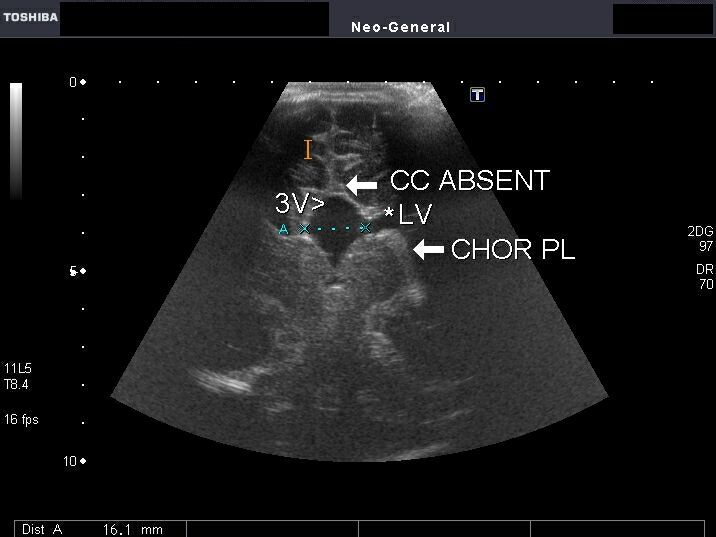
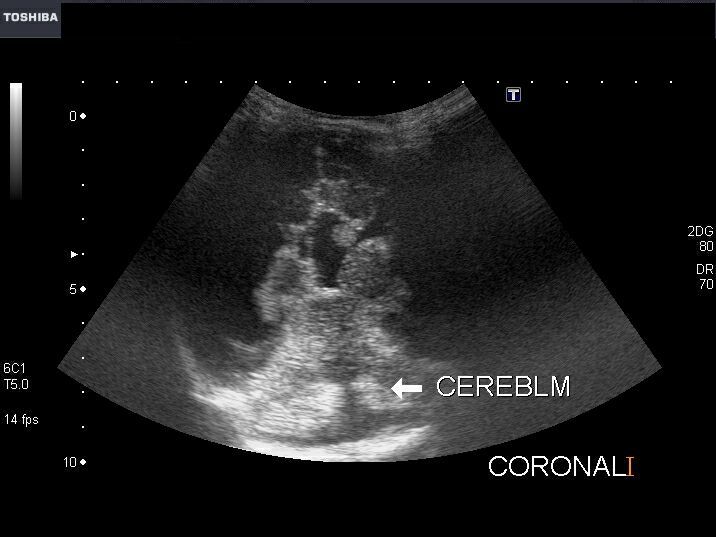
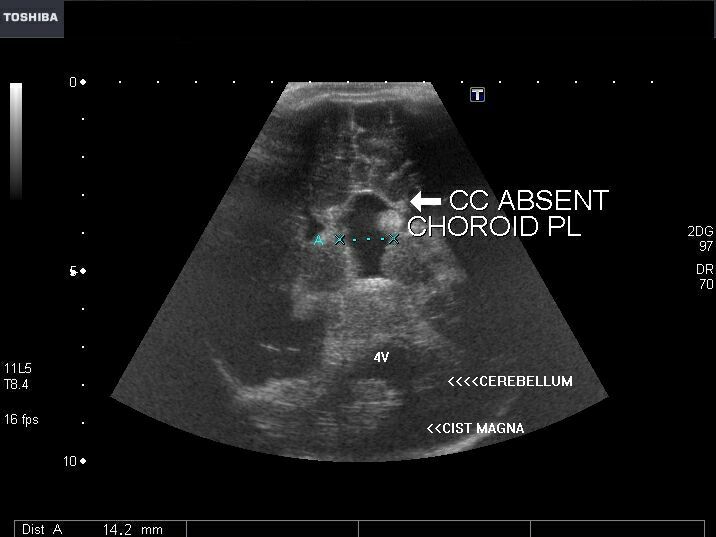
This young female neonate presented with infantile spasms and anophthalmia. Sonography of the brain revealed a) absence of the corpus callosum b) prominent, dilated and elevated 3rd ventricle c) sharply angled lateral peaks of the lateral ventricles which lie far apart d) colpocephaly- prominence of the occipital horns of the lateral ventricles e) echogenic mass in the medial part of the lateral ventricles (Probst bundles) f) posterior fossa cyst which communicates with the dilated 4th ventricle with agenesis of the cerebellar vermis (DANDY WALKER MALFORMATION). These ultrasound images suggest agenesis of the corpus callosum, as part of the AICARDI syndrome. Ultrasound images by Joe Antony, MD, using a Toshiba Xario ultrasound machine.
Reference:
1) http://emedicine.medscape.com/article/941426-overview(free article on Aicardi syndrome)
2) Agenesis of the corpus callosum (free article).
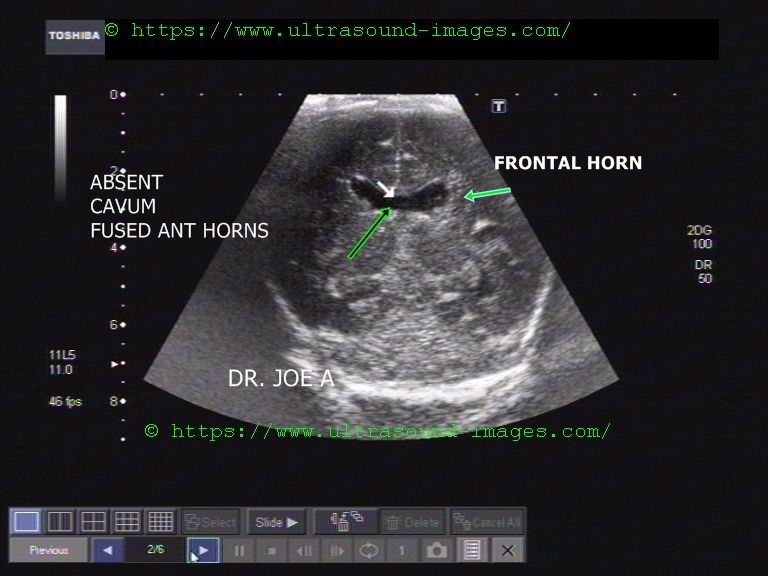
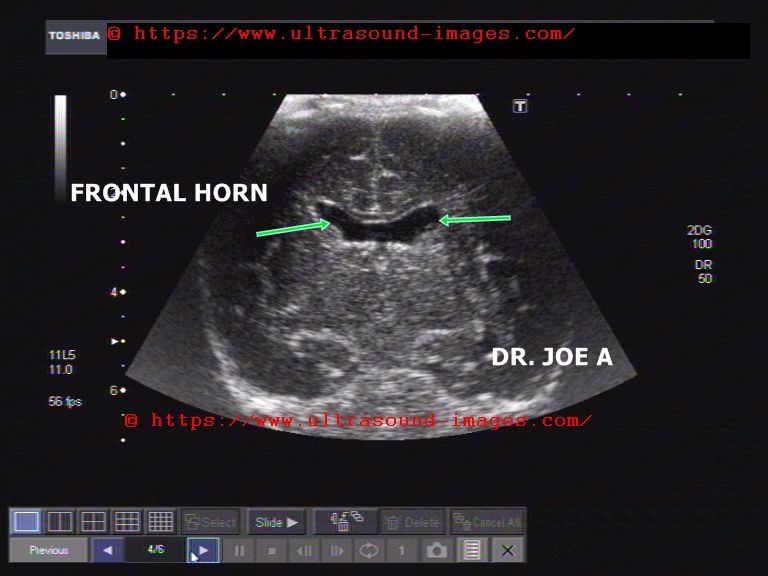
Lobar Holoprosencephaly with partial agenesis of corpus callosum


Sonography of this neonatal brain shows- fusion of the anterior horns of both lateral ventricles with absent cavum septum pellucidum. The corpus callosum is partially deficient. These ultrasound images suggest partial agenesis of the corpus callosum in a case of Lobar Holoprosencephaly. The cerebral hemispheres are otherwise well preserved. Images were taken using a Toshiba Xario Ultrasound and Color Doppler system by Joe Antony, MD.
Reference: http://emedicine.medscape.com/article/409265-overview
Periventricular leukomalacia in neonate




Multiple minute cystic lesions in white matter
This preterm neonate underwent sonography of the brain. Ultrasound images of the infant's brain revealed multiple small cystic lesions (2 to 3mm. size) the periventricular part of the deep white matter. Color Doppler image did not show any specific findings. These ultrasound appearances are diagnostic of Periventricular leukomalacia in the neonate's cerebral hemispheres. Periventricular leukomalacia can also present as markedly hyperechoic white matter. This condition is the result of chronic ischemic insult (chronic ischemia) of the infant's brain during immediate postnatal period (in preterm neonates).
Reference:
http://emedicine.medscape.com/article/975728-overview (free article and images)
http://emedicine.medscape.com/article/416016-imaging(free article and images)
Cerebral edema in neonate
A) Coronal section of normal neonatal brain

The normal neonatal brain is seen in coronal section using high resolution ultrasound (image above). The image shows the lateral ventricles, the cavum septum pellucidum (the anechoic space between the frontal horns of lateral ventricles) and the interhemispheric fissure. Note the normal width of all these structures
B) Severe cerebral edema in neonate

This neonate (ultrasound images above) shows typical features of severe cerebral edema. These include effacement of the cerebral sulci and gyral pattern, effacement of the interhemispheric fissure (between the cerebral hemispheres) and slit-like lateral ventricles due to expansion (edematous) of the cerebral hemispheres. The cerebral echogenicity also shows diffuse increase. (Please compare with normal neonatal brain- see coronal section -A).
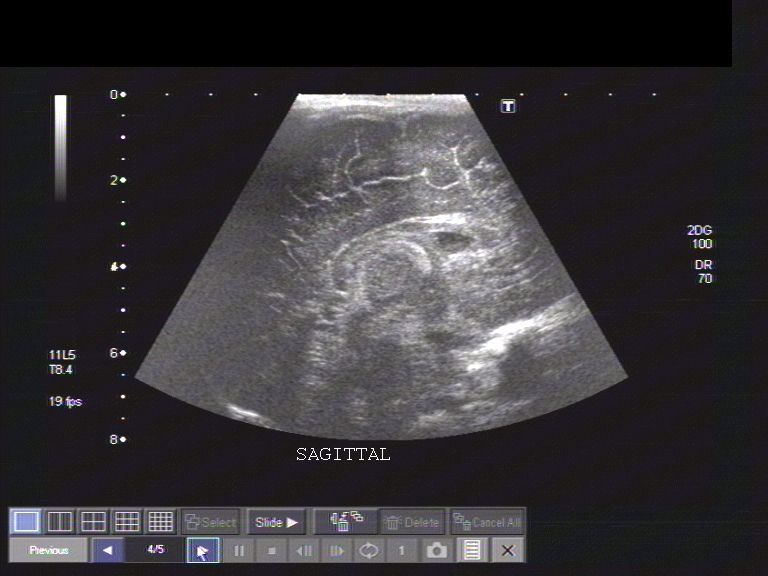
C) Mild cerebral edema in neonate
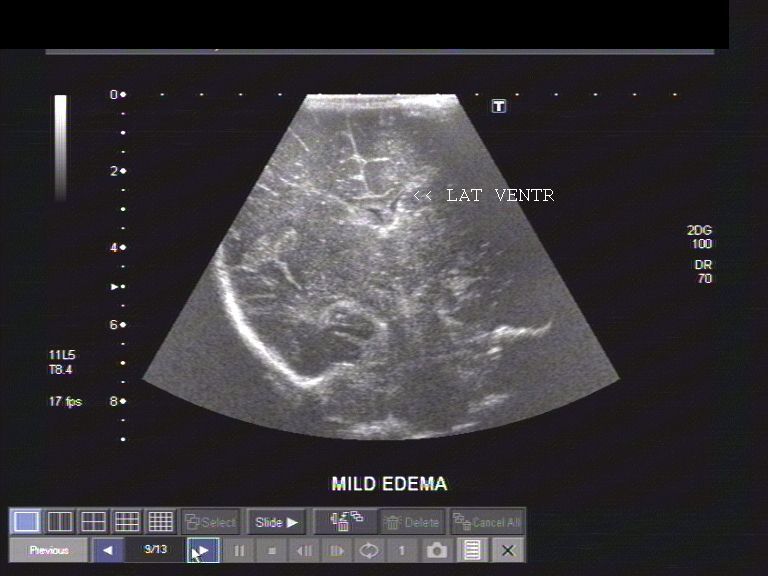
The above ultrasound image shows mild cerebral edema. This neonate shows partial compression of the lateral ventricles. All the features described in section B (severe edema) are seen in a milder form in this image. The interhemispheric fissure is seen but is compressed.
Reference:http://www.ajronline.org/cgi/reprint/176/4/995 (free article and images- excellent)
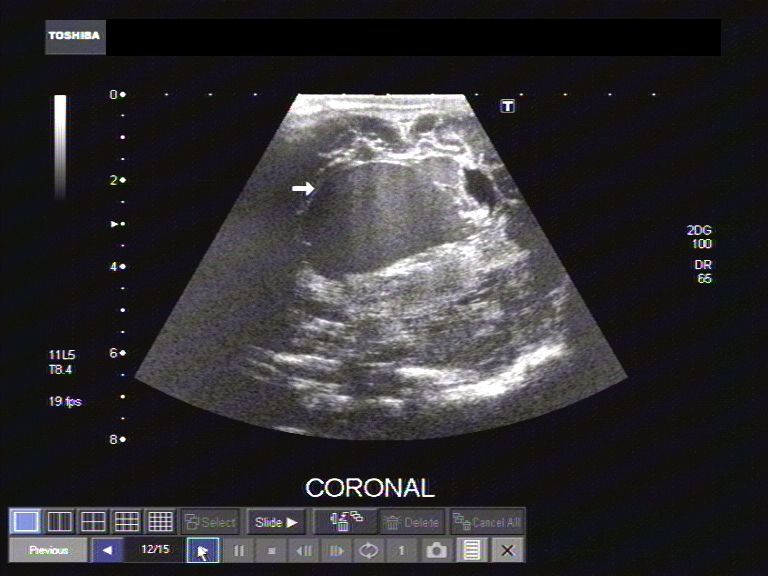
Vein of Galen malformation in neonate (synonym: vein of Galen aneurysm)
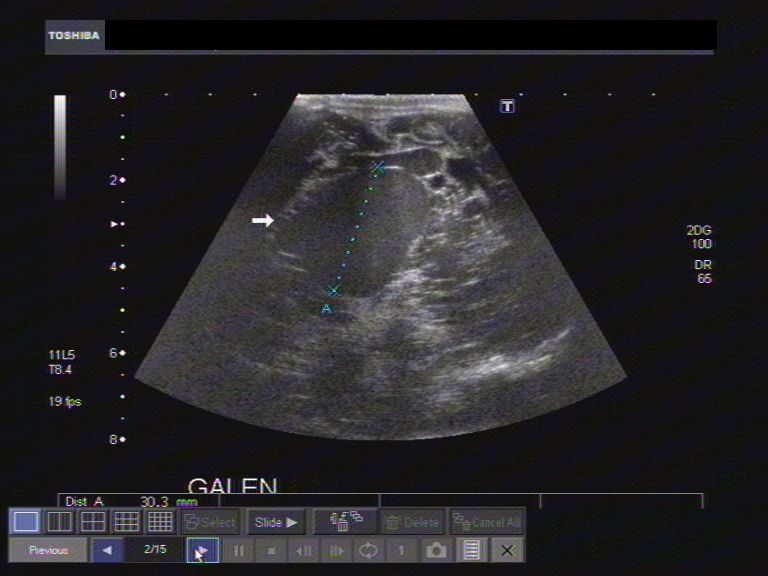
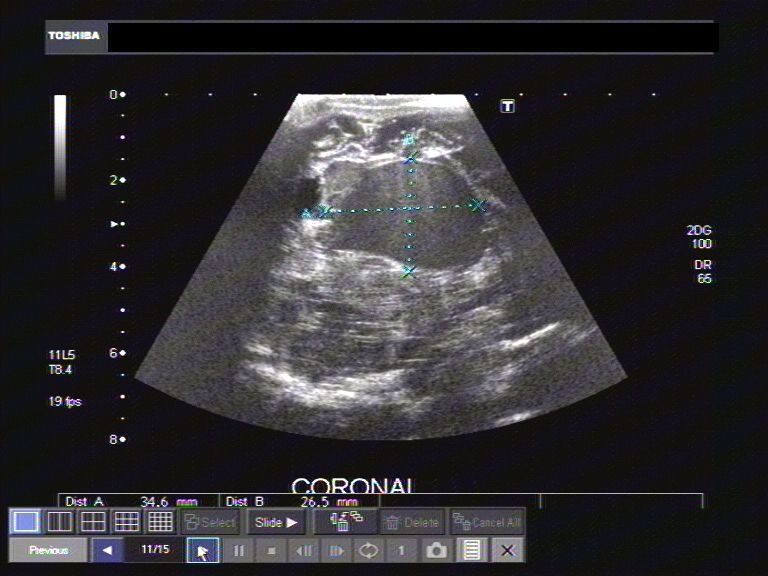
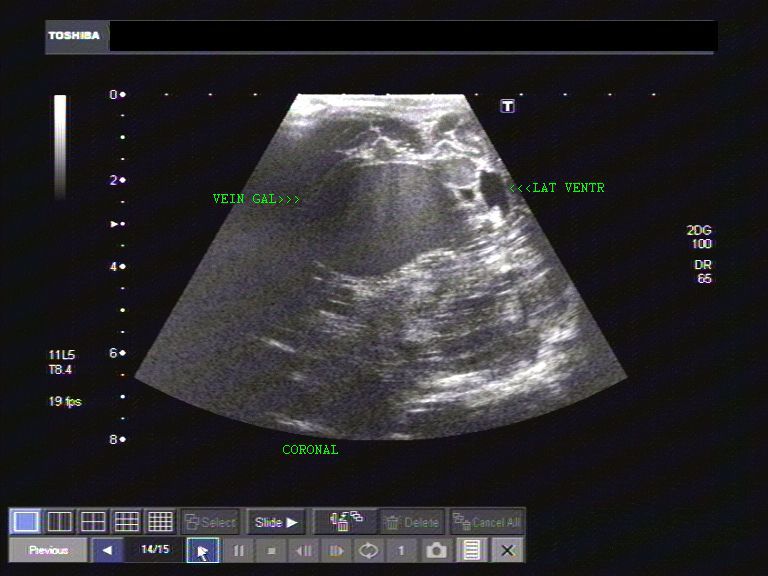
This neonate shows a midline hypoechoic (almost anechoic) space occupying lesion in the supratentorial region of the brain. The above ultrasound images show a coronal section through the neonatal brain. The ipsilateral lateral ventricle appears effaced with the other lateral ventricle displaced.
coronal ultrasound images of the SOL within the neonatal brain.
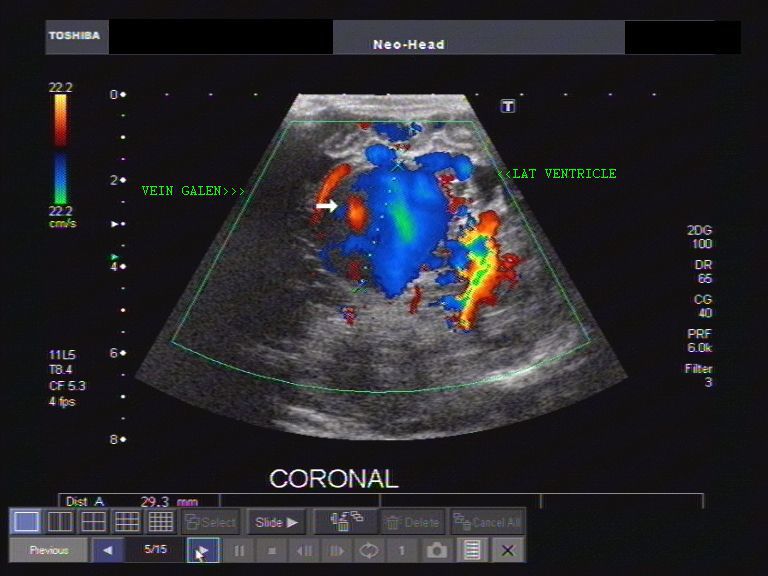

vascular nature of the flow within the SOL (space occupying lesion). The appearances suggest multiple feeder vessels supplying a large midline vessel, a typical appearance of vein of Galen malformation or vein of Galen aneurysm.
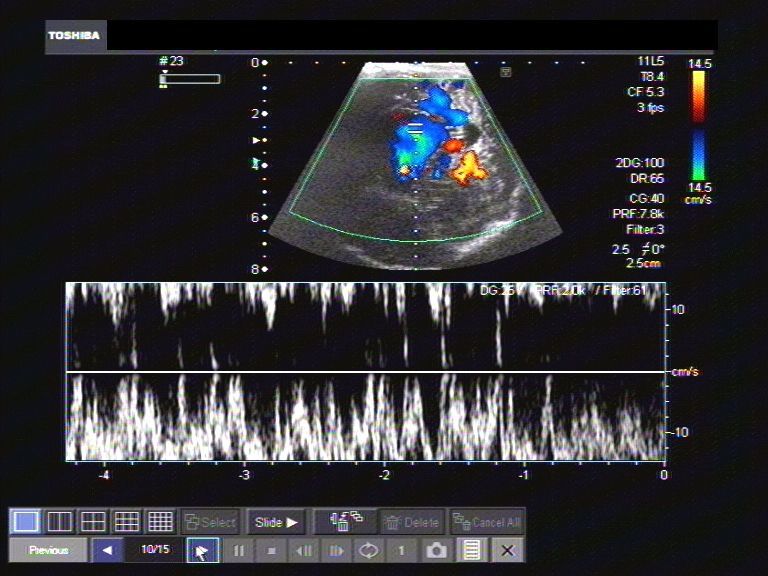
Spectral Doppler study of the vascular SOL in this neonates brain suggests turbulent flow within it. These ultrasound and Color Doppler images are diagnostic of a vein of Galen aneurysm.
References: http://www.jultrasoundmed.org/cgi/reprint/22/12/1395.pdf
Intraspinal cystic lesion in lumbo-sacral region -of neonate (filar cyst vs. ventriculus terminalis)



This neonate showed a sacral cutaneous dimple. Ultrasound images of the lumbo-sacral spine show a cystic lesion of about 1.0 cms. extending from the terminal part of the spinal cord (L-5 downwards). The cyst is elongated and shows clear fluid with no evidence of solid tissue within it. Cystic lesions of this type in the terminal part of the spinal canal are usually ventriculus terminalis. This is typically a long cyst that extends from the tip of the conus medullaris to the filum terminale of the spinal cord. Another cystic lesion which can give similar appearances is the filar cyst, a cyst of the filum terminale. Both these cysts are considered as normal variants, and usually are self limiting and regress with time. Also possible in this case is an arachnoid cyst. Above ultrasound images of ventriculus terminalis / filar cyst are courtesy of Mr. Shlomo Gobi, sonographer, Israel.
References:
http://neuroradiologyonthenet.blogspot.com/2010/09/filar-cyst.html(free blog article)
http://bjr.birjournals.org/cgi/reprint/75/892/384(free article and images)
meningitis-neonate

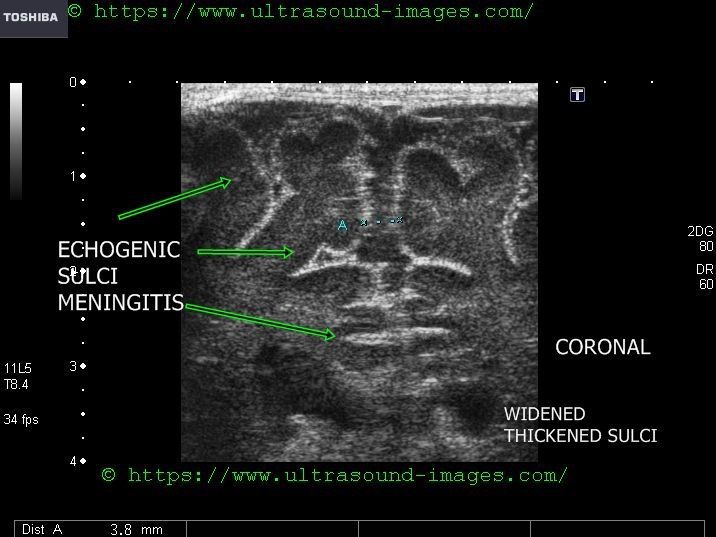
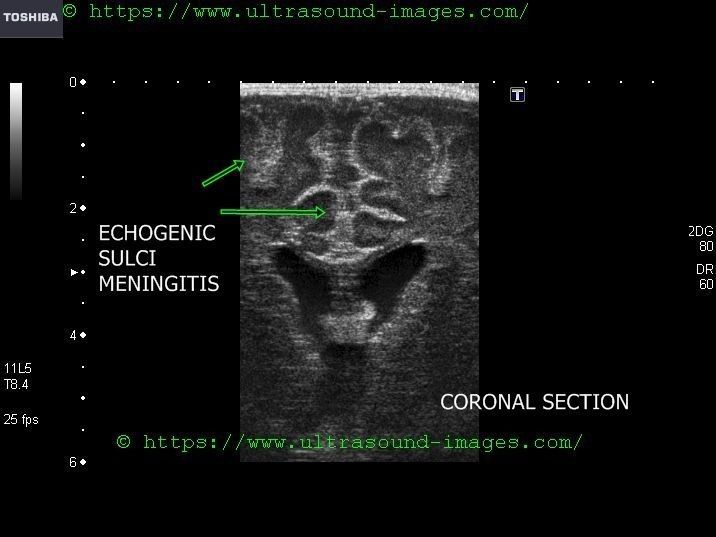

Ultrasound imaging of meningitis in neonate: (see ultrasound images above):
- thickened sulci with widening of sulci
- increased echogenicity of sulci
- hydrocephalus may be present
- thickening of ependymal layer of the ventricles may be present
- widening of sub-arachnoid spaces
- intra- ventricular debris and strands may be present
- increased vascularity or hyperemia of meninges and sulci may be present
- References: sonography of meningitis in neonates
intraventricular-debris-ventriculitis
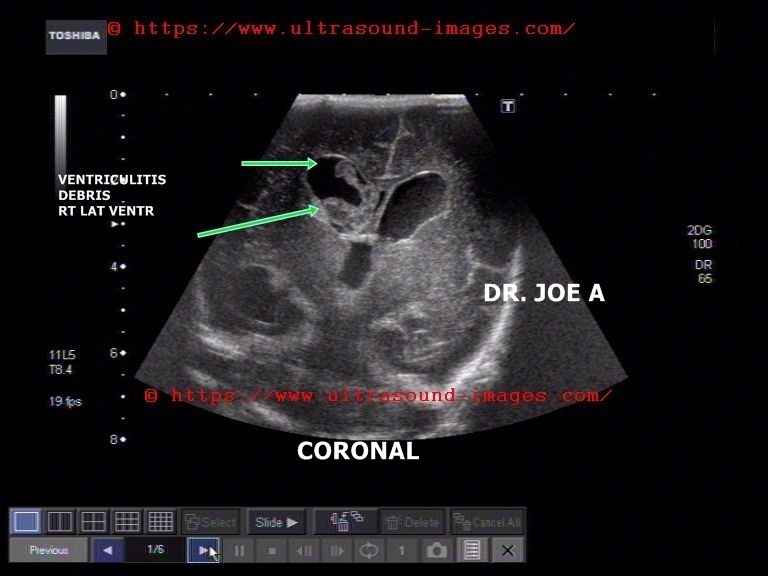
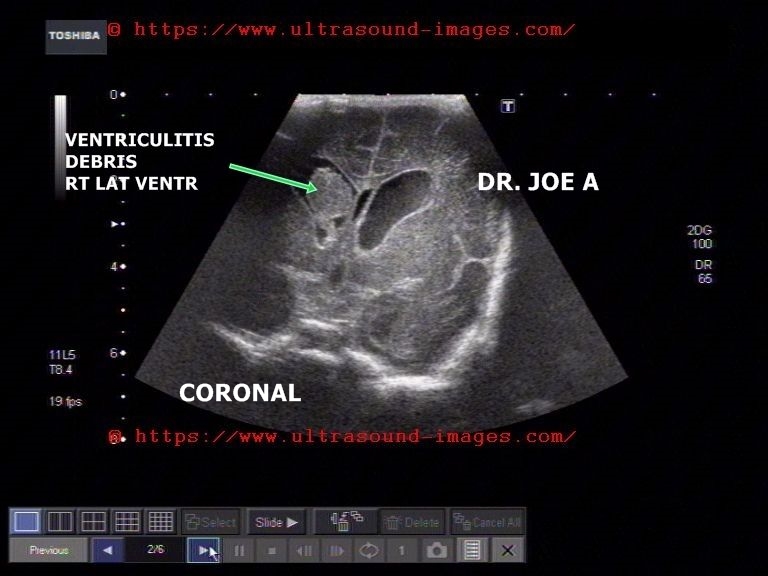
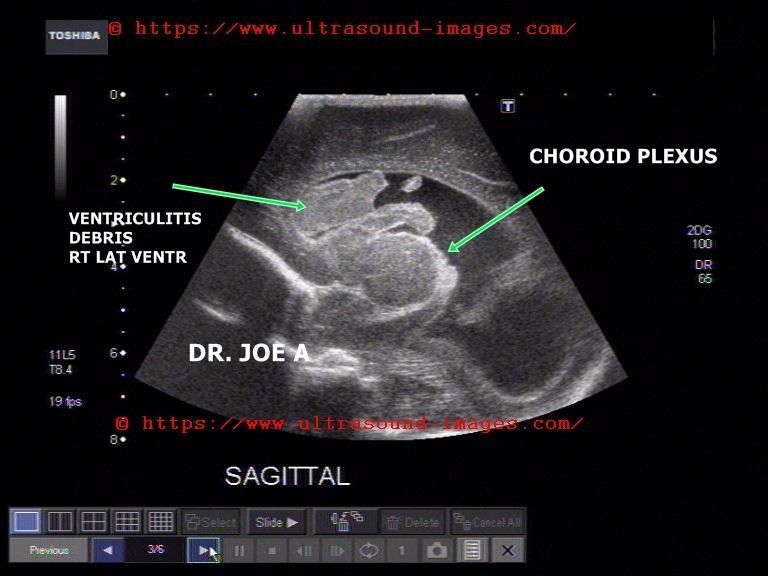
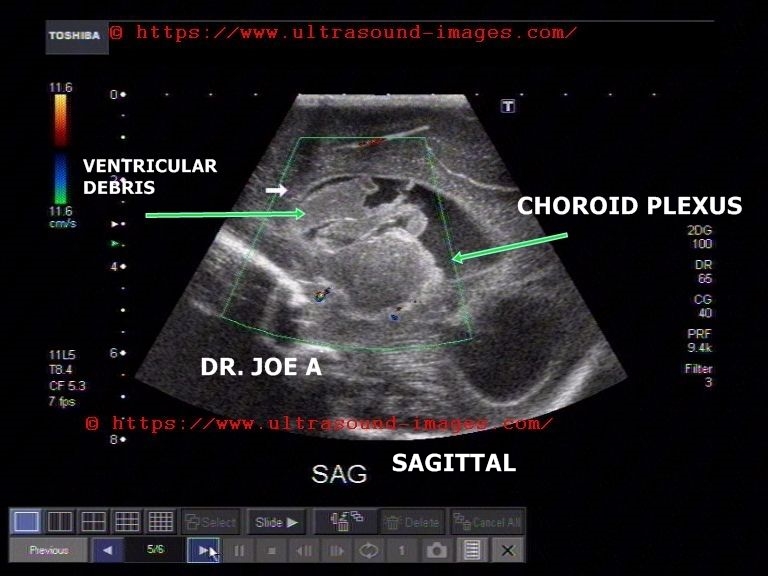
This neonate was markedly febrile.
Ultrasound images of the neonatal brain (transcranial ultrasound) show:
- echogenic debris in Rt. lateral ventricle
- irregular choroid plexus
- dilated lateral ventricles (ventriculomegaly)
- particulate matter in CSF within neonate's ventricles
All these ultrasound findings suggests intracranial bacterial or fungal infection s/o ventriculitis
Later stages of venticulitis may show adhesions within the ventricles.
D/d: similar features may also be seen in intra-ventricular hemorrhage.
Thus clinical history is important.
References: sonography of ventriculitis in neonate
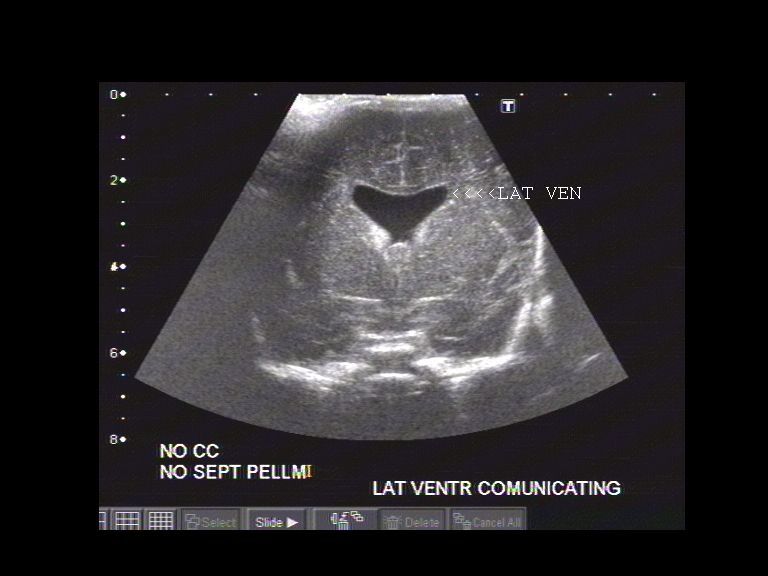
absent-septum-pellucidum
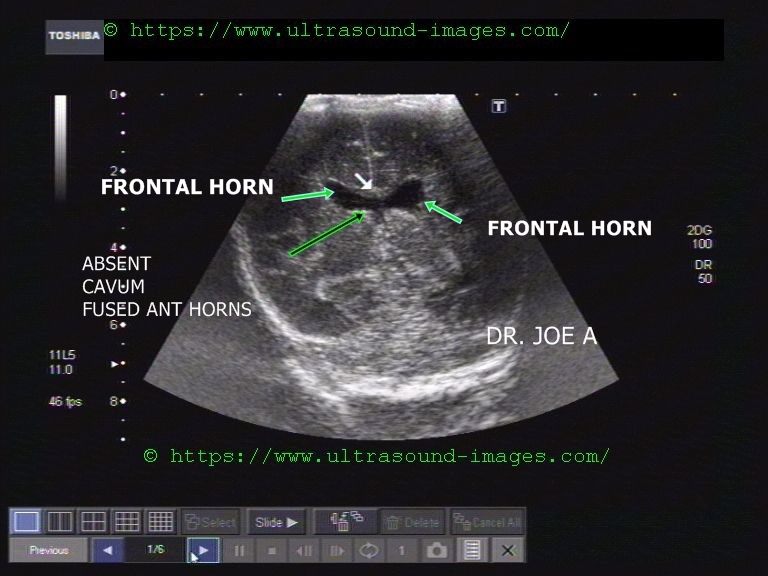

This neonate shows typical features of absent septum pellcidum (transcranial ultrasound imaging):
- the septum pellcidum is not visualized between the frontal horns of the lateral ventricles
- frontal horns of lateral ventricles freely communicate in absence of septum pellcidum
- there is boxing of the frontal horns with marked downward extension of horns.
- this condition is seen usually assoicated with syndromes such as septo-optic dysplasia (hypoplasia of optic nerves + cavum septum pellcidum) and also in lobar holoprosencephaly. Also seen in corpus callosum agenesis.
- In small minority of cases absent septum pellcidum is an isolated finding.
- in later age there is high likelihood of schizophrenia
- incidence of 2 to 3 per 100,000 persons
References: sonography of absent septum pellucidum in neonates
© 2026, Joe Antony, MD All images and content in this site are copyrighted. www.ultrasound-images.com When visiting this site, we may use cookies to improve the performance of this site. Use of this site means you accept the use of cookies. Read our privacy policy at this page: https://www.ultrasound-images.com/privacy-policy/