
Ultrasound images of anomalies of the fetal heart
Contents of this page
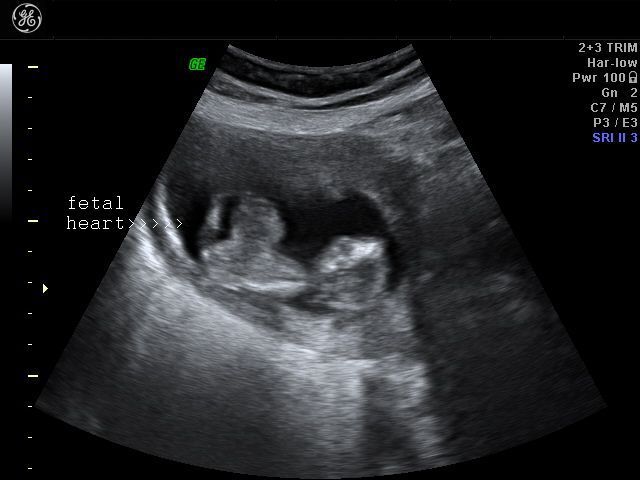
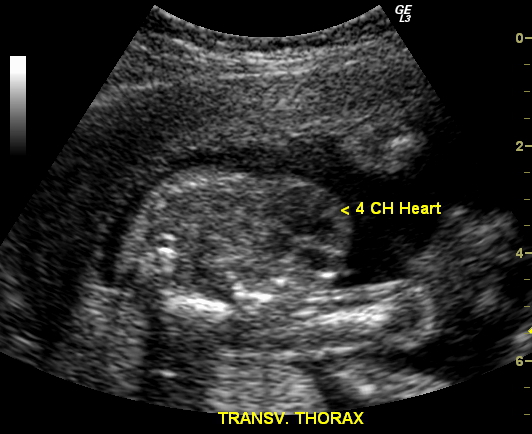
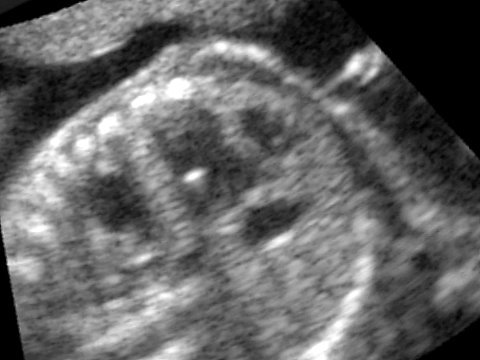
- Normal four chamber view of the fetal heart
- Congenital anomalies of the fetal heart
- VSD (Ventricular Septal Defect)
- Some more Color Doppler/ Ultrasound image of Fetal VSD
- Ectopia cordis
- EIF (Echogenic intracardiac foci)
- Tricuspid dysplasia
- Hypoplastic left heart syndrome
- pentalogy of cantrell
- fetal pericardial effusion
- absent pulmonary valve syndrome
- fetal aortic aneurysm
- fetal right aortic arch
- coarctation of aorta in fetus
- double aortic arch in fetus
- DORV-double-outlet-right-ventricle-with-AVSD
- dilated-cardiomyopathy-in-fetus
- ARSA-aberrant-right-subclavian-artery
- truncus-arteriosus-fetal-echo-STIC
- VSD-STIC-ultrasound
- atrial-septal-aneurysm
Normal four chamber view of the fetal heart
Fetal echocardiography



Download my E book for Amazon Kindle (download free Kindle reader for i Phone or Android)
Assorted ultrasound cases- by Joe Antony, MD
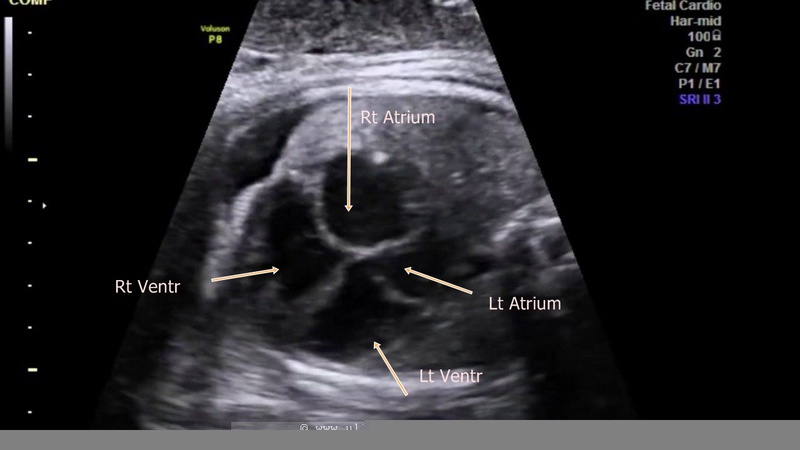
showing normal view of the fetal heart
The above fetal echocardiography images show the normal fetal heart. Note the foramen ovale opening to the left atrium. LA= left atrium
Congenital anomalies of the fetal heart
AVSD (atrioventricular septal defect)

There is a ventricular septal defect involving the upper part of the septum.A large atrial septal defect (ASD) is also seen in these ultrasound images.
The single large AV valve replacing the Mitral and Tricuspid valves
AVSD is also known as endocardial cushion defect or AV canal defect. It is caused by poor or faulty development of the endocardial cushion. These fetuses usually have other associated cardiac anomalies. The above images reveal large defects in the atrial and ventricular septae with a single large Atrio-ventricular valve replacing the mitral and tricuspid valves. In fact the the ASD is so large, that it appears like a single large atrium. Images courtesy of Dr. Latha Natrajan, Bangalore, India.
Reference: http://www.centrus.com.br/DiplomaFMF/SeriesFMF/18-23-weeks/chapter-04/heart/heartfmf-complete.html (free article with video clips and images)... rated (by us) as excellent.
Ultrasound video (fetal echo video) of AVSD: http://www.ultrasoundlink.net/avsd (fetal medicine foundation)
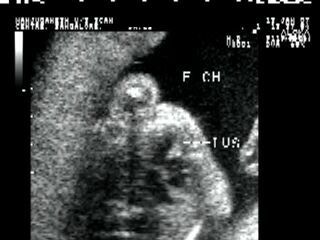
Fetal pericardial mass

Sonography of this 36 weeks old fetus revealed a large echogenic mass in close relation to the exterior of the fetal left ventricle, within the pericardial cavity.. A small pericardial effusion is also present. These ultrasound images suggest a solid, non-calcific mass of the pericardium. Possibilities include rhabdomyoma, teratoma and hemangioma. Rhabdomyomas are the commonest pericardial tumours and account for almost 75 % of cardiac masses. Teratomas can be either cystic or solid. Image courtesy of Dr. Prathima Radhakrishnan, Bangalore, India.
Reference:
1) Pericardial Hemangioma Presenting as Thoracic Mass in utero (abstract)
DORV (Double Outlet Right Ventricle)
This is a 4.2 MB video file in GIF format. It might take some time to download. The aorta and the pulmonary trunk are seen mostly arising from the right ventricle. This condition is difficult to distinguish from Fallot's tetralogy and Transposition of the great arteries (TGA). Video courtesy of Dr. Latha Natrajan, Bangalore, India.
References: Fetal echocardiography video of Double outlet right
ventricle: http://www.ultrasoundlink.net/double-outlet-right-ventricle-dorv-echo (fetal medicine foundation)
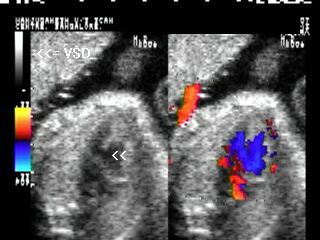
VSD (Ventricular Septal Defect)
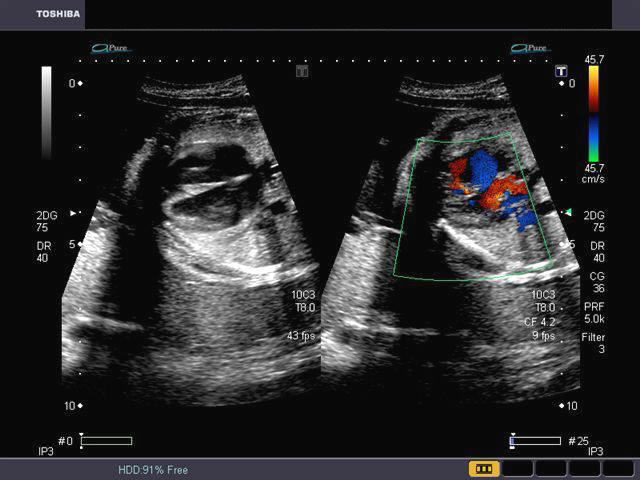


Sonography of fetal VSD.
These ultrasound and color Doppler images show a VSD in the muscular part of the ventricular septum of the fetal heart. This type of VSD is called a ventricular septal defect. Flow is seen across the defect in the septum, from left ventricle to the right (color Doppler images). There are 4 types of VSD:
a) perimebranous b) inlet c) trabecular d) outlet. This classification is based on the location of the defect. Images courtesy of Gunjan Puri, MD, India.
See this link for more: Fetal echocardiography (free article and images). Rated excellent..
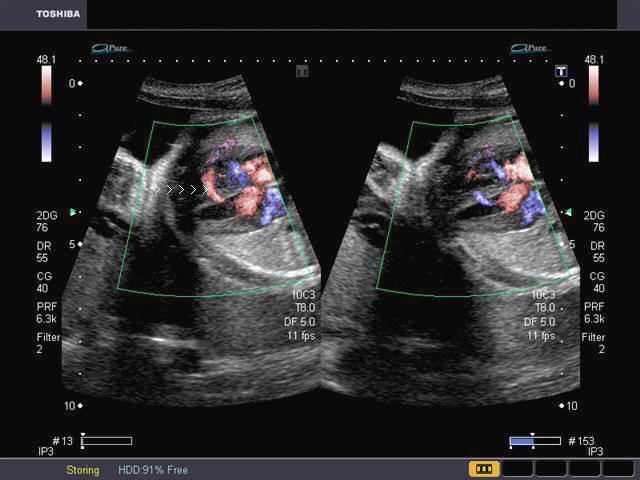
Some more Color Doppler/ Ultrasound image of Fetal VSD
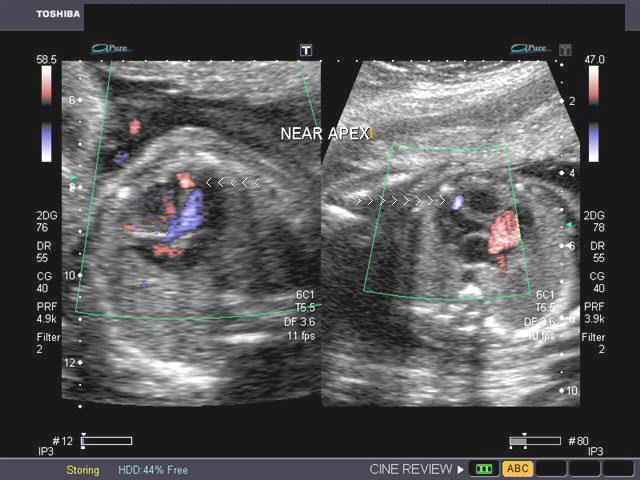

This 3rd trimester fetus showed a small Ventricular Septal Defect (VSD) (see arrow heads), near the cardiac apex. Flow across the septum is seen in red hue on Color Doppler imaging (arrowheads). Fetal echocardiography images of VSD are courtesy of Gunjan Puri, MD, India.
Ultrasound video (fetal echo) of fetal VSD: www.ultrasoundlink.net/ventricular-septal-defect-VSD-in-fetus (fetal medicine foundation)
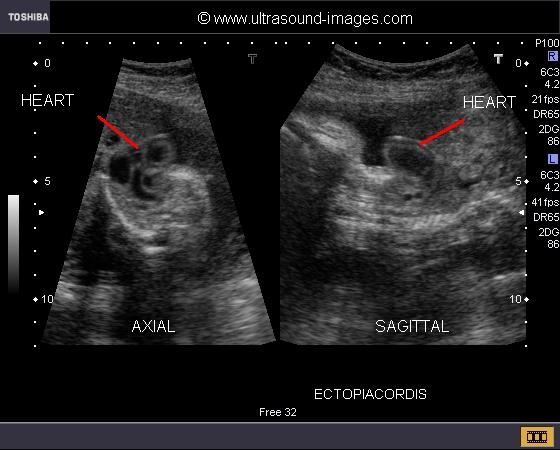
Ectopia cordis
Case-1

Case-3: ectopia cordis in 8 weeks fetus- ultrasound video
There is also a bilateral jugular lymphatic sac observed in this fetus.
The fetal heart lies entirely outside the confines of the thoracic cage.
The above 3 B-mode ultrasound images show the fetal heart lying partially outside the thoracic cage (case-2) or completely outside the thorax (case-1). I have added a video (ultrasound) clip of case-1 at my blog:
See: http://cochinblogs.blogspot.com/2009/09/another-case-of-ectopia-cordis.html
Case 1 does resemble an umbilical hernia from the ultrasound images on top. However the Color Doppler image of case 1 clinches the diagnosis of ectopia cordis. This was a early 2nd trimester fetus. Case-1 ultrasound images are courtesy of Dr. Dilraj Gandhi, India. This fetus also shows increased Nuchal thickness.Case-2 shows ectopia cordis with heart partially ouside the thoracic cage.
The ultrasound video of this case can be viewed at this link http://cochinblogs.blogspot.com/2009/04/ultrasound-video-of-ectopia-cordis.html.
This ultrasound image was taken by Joe Antony, MD,India.
Reference:http://www.thefetus.net/page.php?id=45 ( you can read more at this link)
Fetal echo video of ectopia cordis: http://www.ultrasoundlink.net/ectopia-cordis-pentalogy-of-cantrell(fetal medicine foundation)
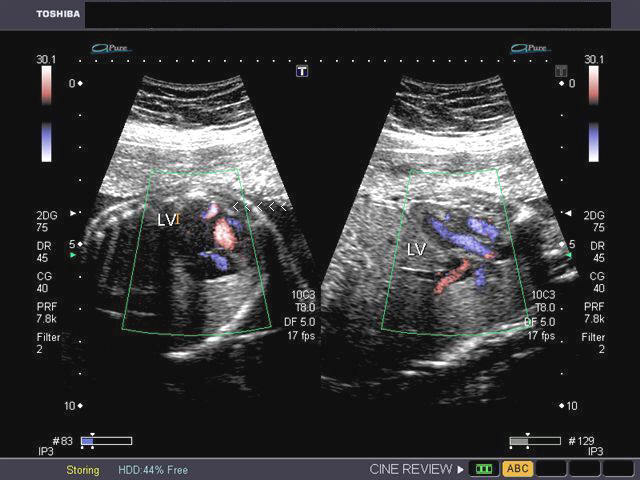
EIF (Echogenic intracardiac foci)
Case 1


Multiple EIF or echogenic intracardiac foci
All three above ultrasound images show echogenic foci in the left ventricle of the fetal heart (3 different cases). The foci are seen in relation to the the chordae tendinae and papillary muscles of the mitral valve leaflets . The overwhelming majority of EIF are seen in the left ventricle and are solitary. The echogenicity of these foci is about the same as that of bone. Echogenic intracardiac foci (EIF) are often seen in Asian fetuses and are usually insignificant. However a small percentage of such fetuses may show associated fetal anomalies and chromosomal anomalies (aneuploidy). You may view a ultrasound video of the EIF in case-1 at: http://ultrasound-images.blogspot.com/
Mutiple EIF:
The ultrasound video above shows two EIF in the fetal left ventricle at 20 weeks.
Multiple EIF are associated with a bad fetal prognosis, like the presence of anomalies and preterm or IUGR and fetal demise.
Reference: http://www.jultrasoundmed.org/cgi/reprint/17/2/127.pdf
Tricuspid dysplasia
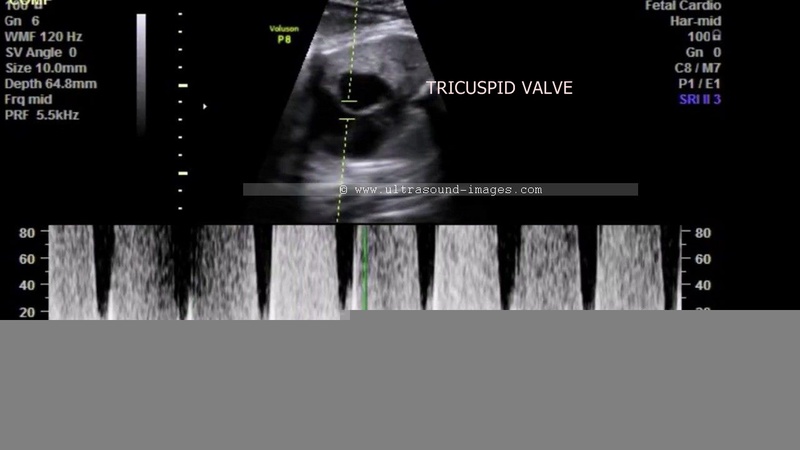
34 week old fetus showing marked thickening and hyperechoic tricuspid valves (arrowed)


LV= left ventricle RV= right ventricle; LA= left atrium; RA= right atrium.
3 Vessel view shows relatively normal pulmonary artery

This 34 week old fetus shows what is called a relatively milder form of tricuspid dysplasia; see the ultrasound and color Doppler images of the fetal heart above. We can see the normal flow across the tricuspid valves as well as the bicuspid valves ruling serious functional problems with this fetal heart. The 3 vessels view also supports this diagnosis of mild tricuspid dysplasia- the normal size of the pulmonary artery supports this diagnosis. The only positive finding in this case is the marked thickening of the tricuspid valve leaflets.
The video of this case of tricuspid dysplasia can be viewed below:
References:
Tricuspid dysplasia- ultrasound imaging
http://www.centrus.com.br/DiplomaFMF/SeriesFMF/doppler/capitulos-html/chapter_12.htm
http://www.ultrasoundlink.net/tricuspid-regurgitation-tr-fetus-12-weeks-of-pregnancy
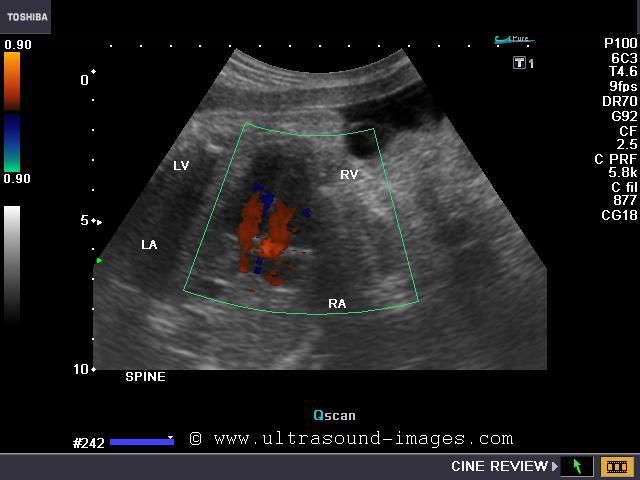
Hypoplastic left heart syndrome


This is a good example of hypoplastic left heart. The main ultrasound findings in this case are a small left ventricle and small left atrium. In addition, the mitral valve is hypoplastic, and hence is barely visualised. In addition, note that the Fetal echocardiogram shows a large and dilated right atrium and right ventricle. The left ventricle is barely visualised and is seen as a small remnant to the extreme left of the fatal heart. The ultrasound video and the ultrasound images above, further confirm that the Fetal ascending aorta and the Fetal aortic valve are small and atretic. Thus, these ultrasound images show a classic picture of hypoplasia of the Fetal left heart, also known as hypoplastic left heart syndrome.
References:
http://www.sonoworld.com/fetus/page.aspx?id=886
pentalogy of cantrell

This second trimester fetus shows (see ultrasound images above) an ectopia cordis with gastroschisis. here the Fetal heart is seen lying well outside the confines of the thoracic wall, with an anterior chest wall defect. The bowel loops are seen freely floating within the amniotic fluid without the covering membrane. This is the typical appearance of gastroschisis. In addition there were also features to suggest disruption of the distal sternumas well as part of fetal diaphragm and also the diaphragmatic pericardium. This group of five ultrasound findings constitute what is known as the pentalogy of Cantrell. These ultrasound images of pentalogy of Cantrell are courtesy of Dr. Durr-e- Sabih, FRCP, Pakistan.
References: 1) ultrasound imaging of pentalogy of Cantrell- sonoworld
2) sonography of pentalogy of Cantrell
case-2-pentalogy-of-cantrell
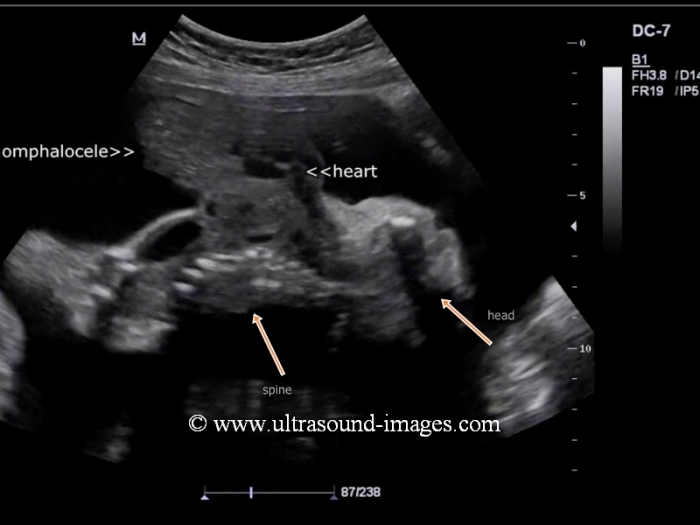

Yet another case of pentalogy of Cantrell (images and ultrasound video are courtesy of Harpreet Kehal, MD). Here, we can appreciate the massive ectopia cordis with almost the entire heart lying outside the thoracic cage, anteriorly with a large omphalocele (containing fetal liver and bowel) also visible. In addition, there also does appear to be a large defect in the diaphragmatic pericardium, the anterior half of the diaphragm as well as the distal sternum. However, these (latter) findings can only be confirmed on autopsy. The prognosis in such major anomalies, like pentalogy of Cantrell is very poor and termination of the pregnancy is possibly the best option, due to the high mortality, even with best medical and surgical care. Ultrasound video of this case is shown below:
fetal pericardial effusion
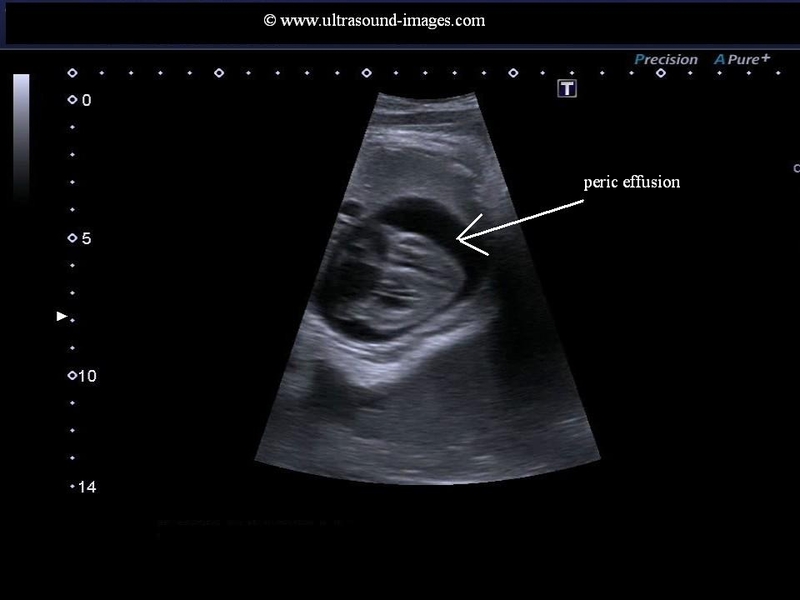
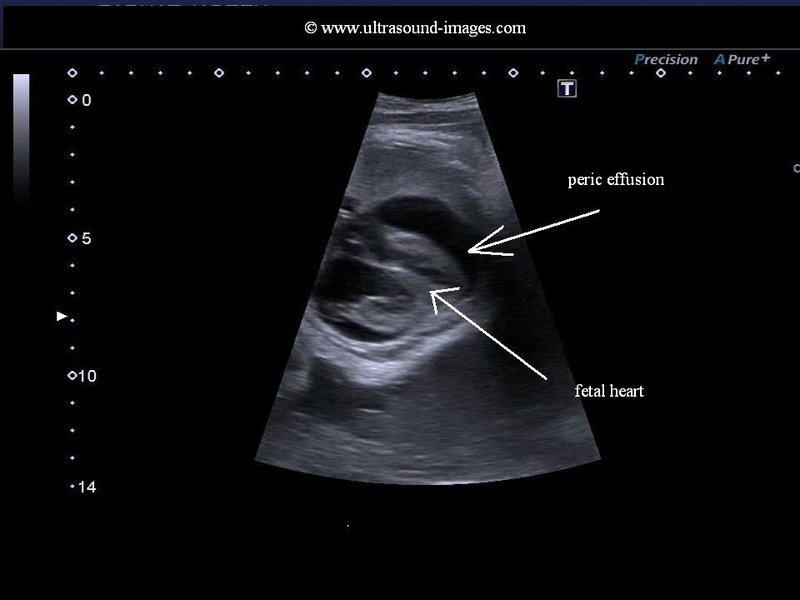
This 35 week old fetus shows a large anechoic fluid collection around with Fetal heart. Fluid collections of more than 2 mm width in the pericardial space is considered as a significant pericardial effusion. The ultrasound images above show severe pericardial effusion in this fetus. Studies suggest however that isolated pericardial effusion without any other Fetal anomalies may not be significant if the width of the Fetal pericardial effusion is between 2 to 7 mm. The greatest risk to the Fetal life is the danger of cardiac tamponade or compression of the Fetal heart due to the pericardial fluid resulting in poor cardiac function.
These ultrasound images of pericardial effusion in fetus are courtesy of Dr. Durr-e-Sabih, FRCP.
References:sonography of Fetal pericardial effusion
fetal-pericardial-effusion-case-2
Another example of fetal pericardial effusion (see fetal echo ultrasound video below). Here there is a moderate pericardial fluid collection in this 19 week fetus. Again, as stated before, isolated fetal pericardial effusion of this type without associated pleural effusion or ascites and without major congenital cardiac anomalies has a good prognosis for the fetus with the periardial fluid collection resolving by the 3rd trimester pregnancy. Hence careful follow up ultrasound scan of the fetal heart is indicated. This ultrasound video of fetal pericardial effusion is courtesy of Dr. Girish Patel, MD.
absent pulmonary valve syndrome


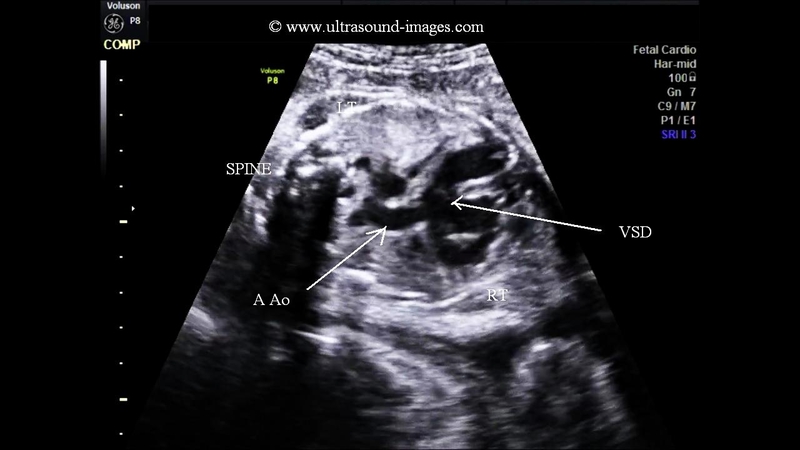
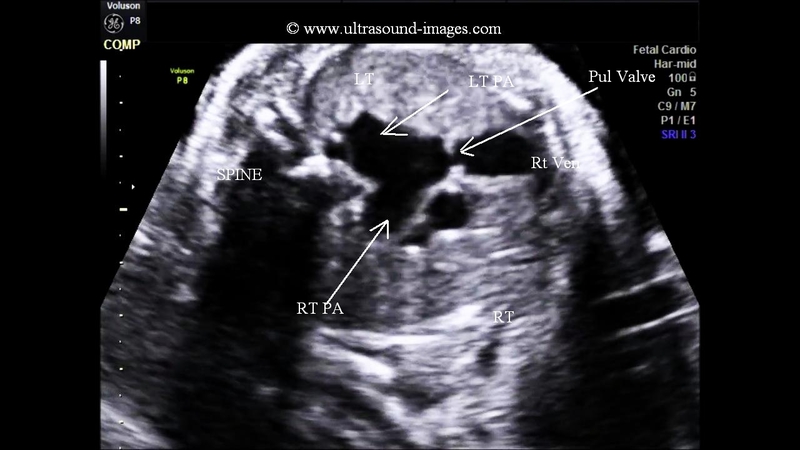

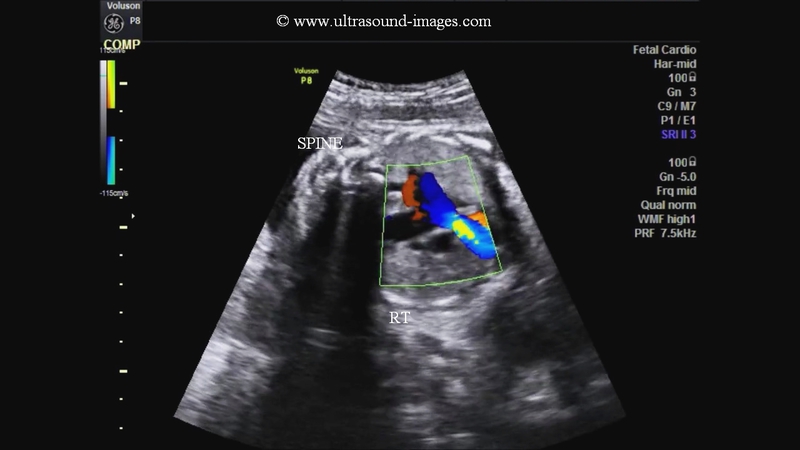
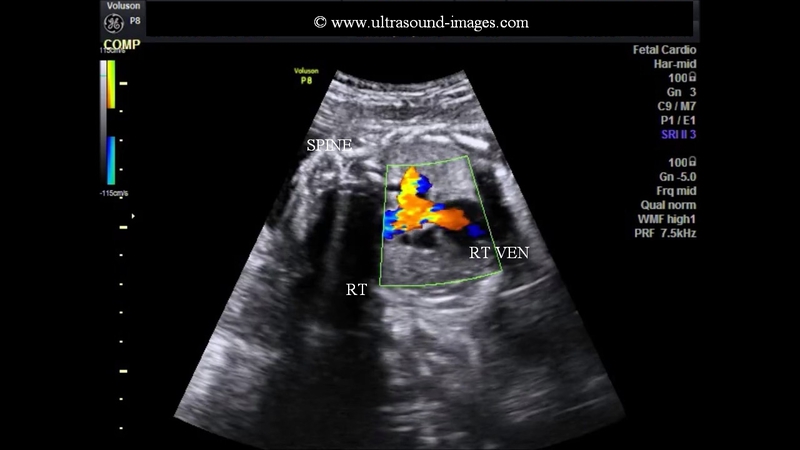
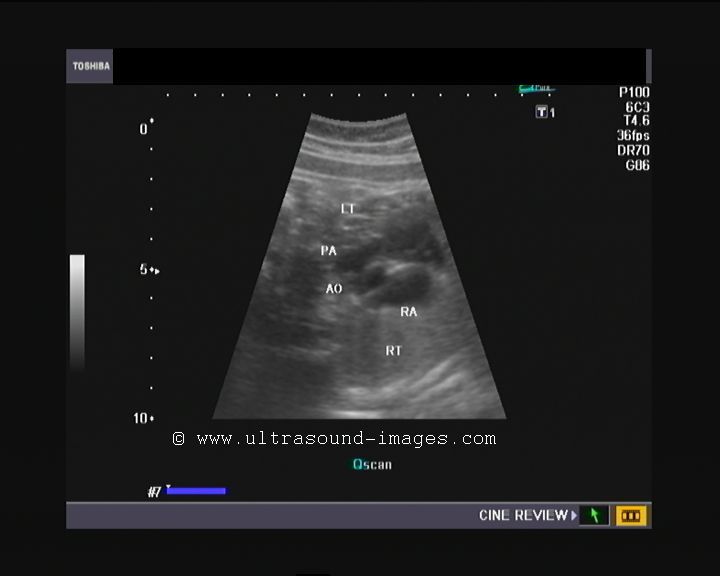
This late second trimester fetus shows multiple cardiac anomalies. The main ultrasound (fetal echocardiography) findings here are:
1. Absent pulmonology valve.
2. Ventricular septal defect.
3. Massively dilated right and left pulmonary arteries.
4. The ascending aorta overriding the ventricular septal defect and both ventricles.
5. Absent patent ductus arteriosus.
6. A distended enlarged right ventricle.
The ultrasound and colour Doppler images provided above display these features and are diagnostic of absent pulmonary valve syndrome. The colour Doppler images of this fetal heart also show turbulent flow across our non-functioning or absent pulmonary valve with to and fro flow from the right ventricle and back to the right ventricle. These ultrasound and color Doppler images of absent pulmonary valve syndrome are courtesy of Dr. Firoz Bhuvar, MD.
Absent pulmonary valve syndrome is described to be a subtype of tetralogy of Fallot. It is characterised by the findings described above and the chief feature is the absence, hypoplasia or non-functioning pulmonary valve in the fetus. There is almost invariably a hugely dilated pulmonary trunk with hugely distended pulmonary arteries. A variant of the absent pulmonary valve syndrome is described in medical literature wherein some of the findings of the syndrome are present and in a milder form. The chief cause of the marked distension of the pulmonary arteries is due to the presence of both stenosis and regurgitation across a non-functioning pulmonary valve.
There is a frequent association with a chromosome 22q deletion in this syndrome.
References:
1. http://sonoworld.com/fetus/page.aspx?id=2820
2. European Journal of echocardiography - article on absent pulmonary valve
syndrome
3. Journal of ultrasound in medicine article on absent pulmonary valve syndrome in fetus
fetal aortic aneurysm




This late second trimester fetus shows a spherical dilatation of the proximal descending aorta near its junction with the fetal arch of aorta.This abnormal dilation of the fetal aorta is characteristic of aneurysm of the aorta. These ultrasound and colour Doppler images of fetal aortic aneurysm are courtesy of
Firoz Bhuvar, MD. fetal aortic aneurysm is a very rare entity and is often associated with various syndromes which involve connective tissue disorders such as Marfans syndrome or Ehler-Danlos syndrome. among the principal differential diagnosis in such a case, are coarcation of the aorta posts stenotic dilation or more often due to kinking of the fetal aorta. These ultrasound images however, did not show any kinking and hence our diagnosis is confirmed.
references:ultrasound imaging of fetal aortic aneurysm
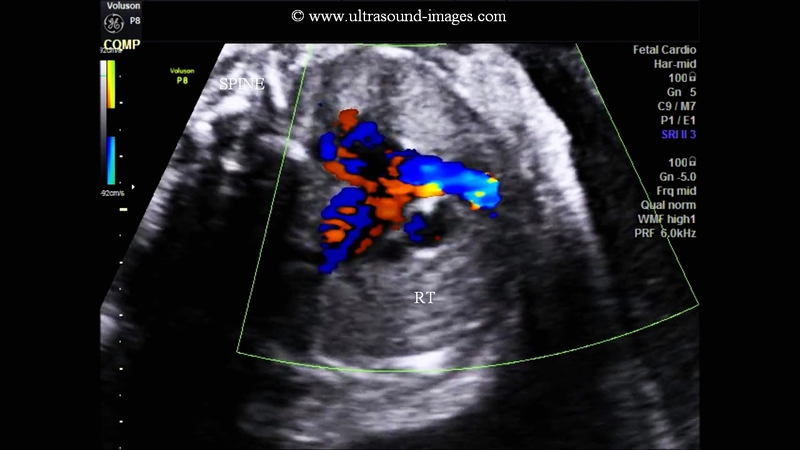
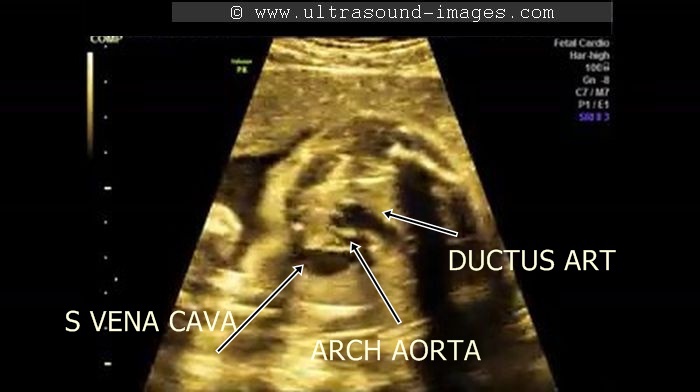
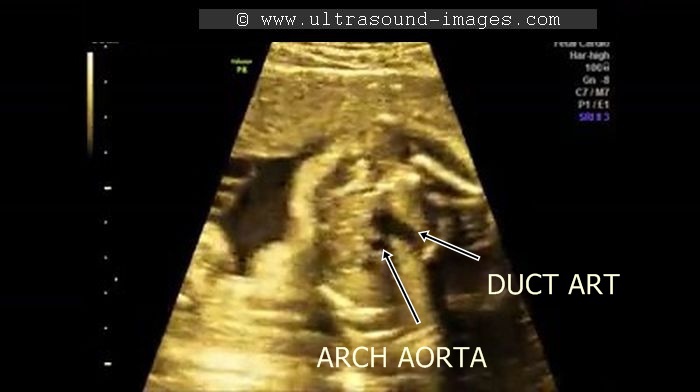
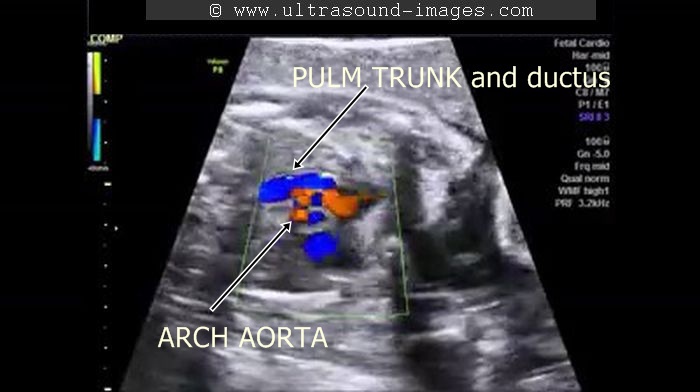
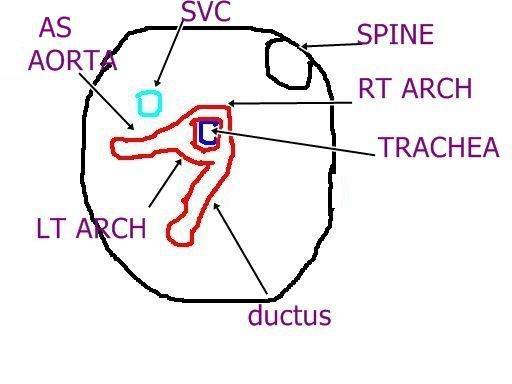
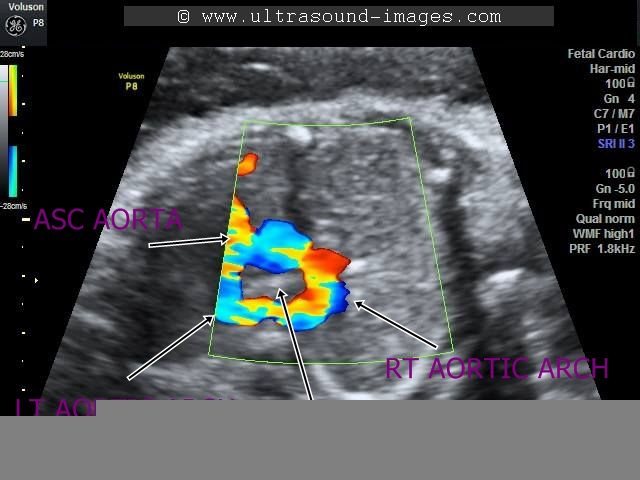
fetal right aortic arch
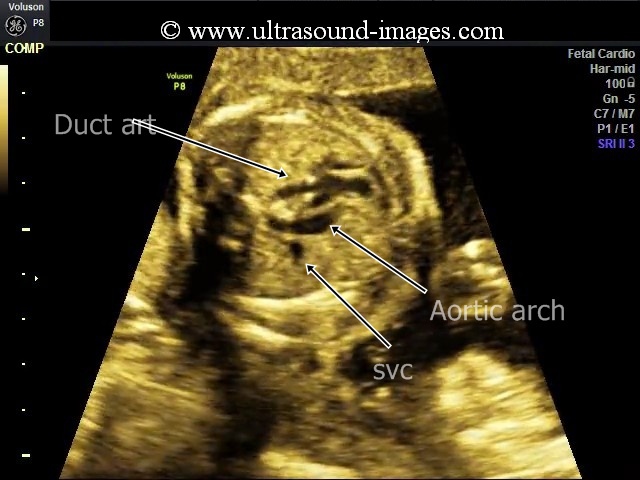

These ultrasound images show a three vessel view of the fetal heart. Can you spot the anomaly in this case? These Fetal echocardiography images show the superior vena cava, the aortic arch, and the pulmonary trunk with the ductus arteriosus proceeding from it. In this case, the Fetal aortic arch is located to the right of the trachea ( shown by the arrow) and also note that the confluence of the aortic arch and the ductus arteriosus is not V shaped ( as is the case in the normal left sided aortic arch) but U- shaped as in this case. All these ultrasound findings point to the fact that this is a normal anatomical variant called the right aortic arch. The right aortic arch is merely located to the right of the trachea and hence receives this name. Ultrasound images of right aortic arch, courtesy of Firoz Bhuvar, MD.
references: sonography of right aortic arch
The fetal echo video above demonstrates the fetal right aortic arch (same case study as the images above)
coarctation of aorta in fetus


Sonography in conjunction with colour Doppler ultrasound imaging is an excellent tool in the diagnosis of coarctation of the aorta in the fetus. However, it must be noted that the demonstration of fetal coarctation of the aorta may be difficult if the pathology is limited to a very narrow segment of the fetal aorta.In cases where a wide segment of the aorta is involved as in tubular hypoplasia of the fetal aorta is present, it is much more easier to image coarctation of the aorta.
in this second trimester foetus, the following ultrasound findings are present (see ultrasound images above):
1. The left ventricle and left atrium appear comparatively smaller than the right ventricle and right atrium.
2. There is a large ventricular septal defect or VSD in this Fetal heart.
3. The Fetal aorta appears smaller in calibre than the Fetal pulmonary trunk and the ductus arteriosus.
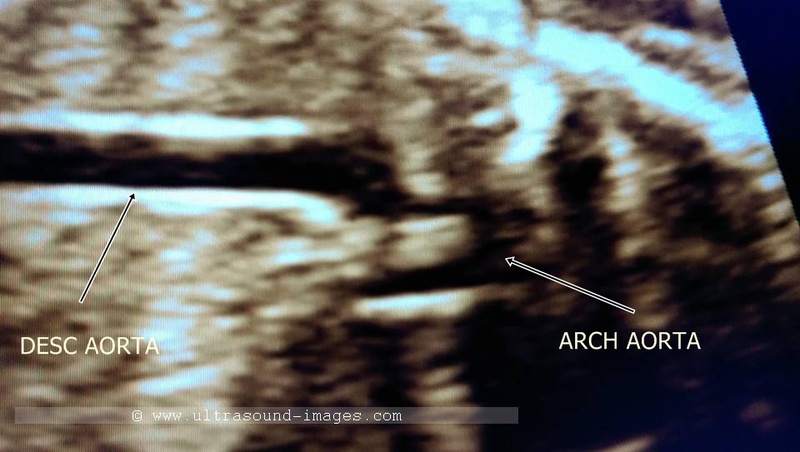
4. The sagittal section ultrasound image of the Fetal thoracic aorta and the arch of aorta shows marked narrowing of the entire arch of aorta till it's junction with the descending thoracic aorta.
All these ultrasound image findings along with the colour Doppler ultrasound image point to a pathology of the Fetal aorta called tubular hypoplasia of the of aorta, which is a subtype of coarctation of the aorta. In tubular hypoplasia of the aorta, a wide segment of the aorta is involved in stenosis, with the arch of aorta usually involved. Classic coarctation of the aorta involves a shelf like constriction of a very narrow segment of the arch of aorta, at the level of the ductus arteriosus. When this construction extends over a wide segment of the aorta it is called tubular hypoplasia of the aorta.
This must be distinguished from other pathologies of the aorta such as aortic stenosis and interruption of the arch of aorta. In aortic stenosis, the left ventricle appears globose and echogenic. In interruption of the arch of aorta, there is a physical discontinuity somewhere within the thoracic aorta usually at the level of the arch of aorta.
These ultrasound images of tubular hypoplasia, (coarctation of the aorta) are courtesy of Firoz Bhuvar, MD.
double aortic arch in fetus


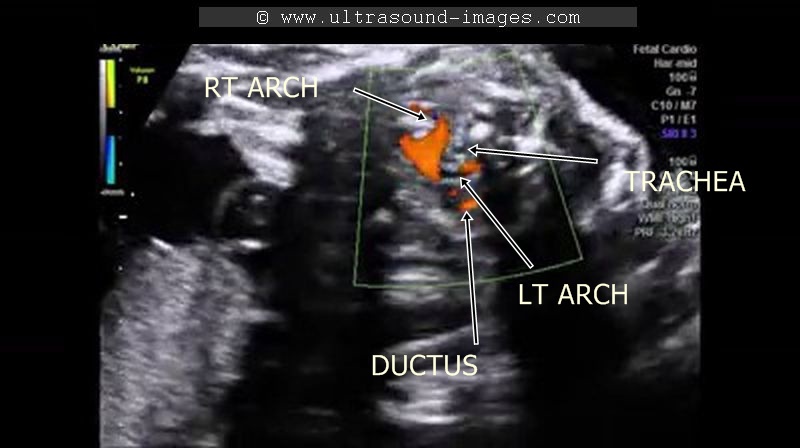
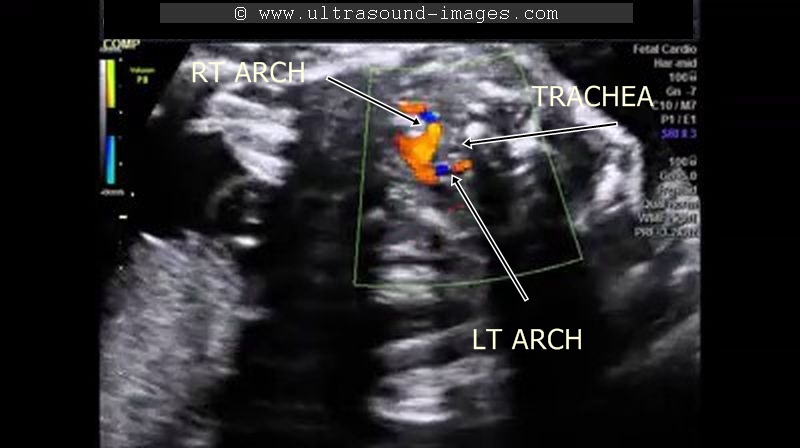


This second trimester fetus shows a division of the aortic arch into two parts- the right aortic arch which courses to the right of the fetal trachea and the left aortic arch which courses to the left of the trachea; both meeting posterior to the trachea and in the process, encircling the trachea in a vascular ring. The left aortic arch is smaller than the right aortic arch, and is possibly atretic. As can be seen in the ultrasound and colour Doppler images above, the left aortic arch is seen to be joined by the ductus arteriosus. these ultrasound images and colour Doppler study images are courtesy of Firoz Bhuvar, MD. In the fetus, the presence of a double aortic arch forming a vascular ring around the trachea may usually not result in major symptoms. However, later on, the vascular ring form by the double aortic arch can cause tracheal compression with resultant airway obstruction.
references:
1. Sonoworld article on sonography of double aortic arch
2. Journal of ultrasound article on ultrasound of double aortic arch
3. American Journal of radiology article on ultrasound imaging of double aortic arch
4. medscape article double aortic arch
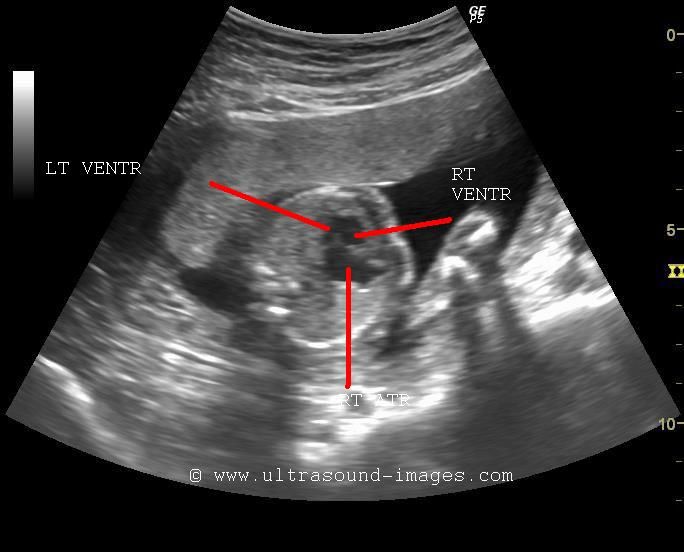
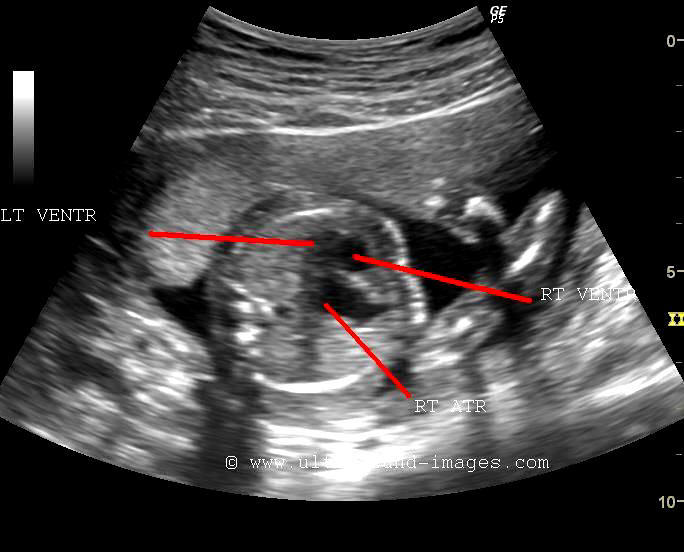
DORV-double-outlet-right-ventricle-with-AVSD






This second trimester fetus shows a number of multiple congenital fetal cardiac anomalies. The first is the presence of AVSD or atrioventricular septal defect. This is characterised by large apical atrial septal defect and a basal ventricular septal defect with an abnormal Common atrioventricular valve. Also note ( see the Fetal echo-images above) an increase in atrial length compared to the ventricular length resulting in an altered atrioventricular length ratio.
another congenital cardiac anomaly present in this fetus is- double outlet right ventricle- wherein both the Fetal aorta and pulmonary trunk or main pulmonary artery both emerge from the Fetal right ventricle. note in these ultrasound images above that the Fetal ascending aorta and the Fetal pulmonary trunk lie parallel to each other. This parallel configuration of the Fetal aorta and the pulmonary trunk is also seen in transposition of the great arteries (TGA). Thus, TGA is one of the chief differential diagnosis of double outlet right ventricle.
In addition, another Fetal cardiac anomaly noted in these Fetal echo- images above is that the main pulmonary artery or pulmonary trunk is narrower than the Fetal ascending aorta. This is due to mild pulmonary stenosis which is common in cases of double outlet right ventricle (DORV). the colour Doppler flow image of the pulmonary trunk confirms this fact by the lack of any aliasing or turbulence in the flow of this vessel. These Fetal echo images and video of DORV with a AVSD with mild pulmonary stenosis are courtesy of Firoz Bhuvar, MD.
References:
1) sonographic imaging and Fetal echo-cardiography of DORV
2)
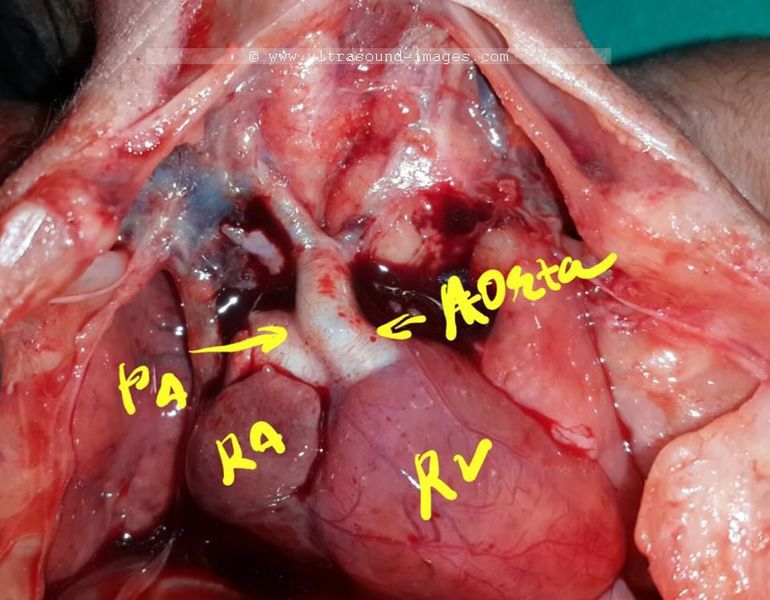
DORV-case-3-STIC


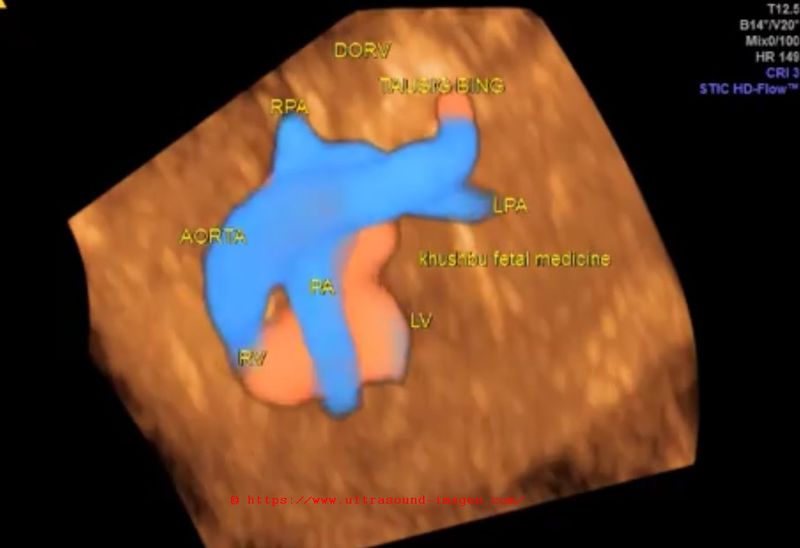
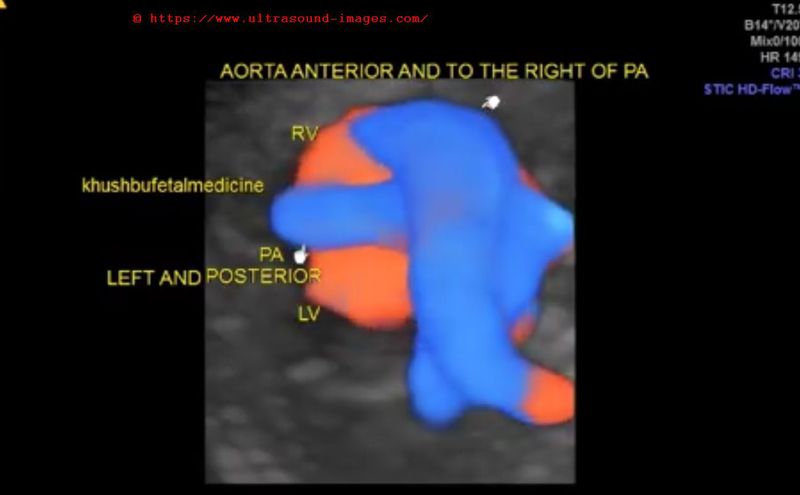
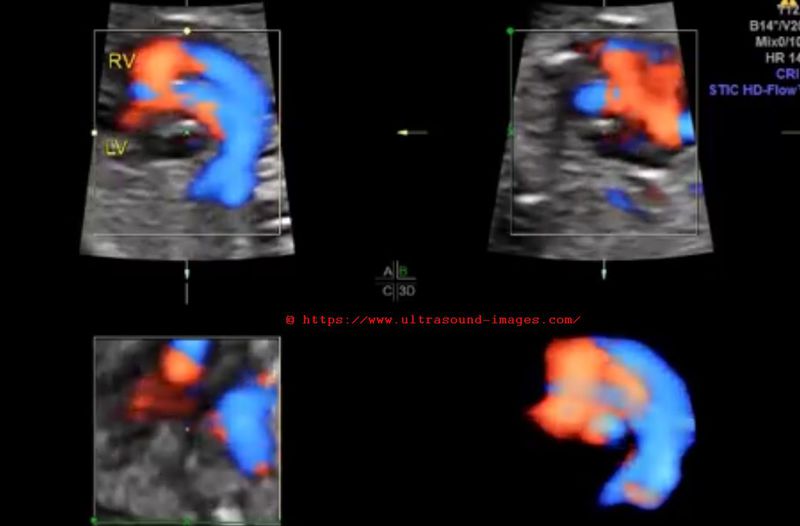
This 2nd trimester fetus shows DORV or double outlet right ventricle with a sub-pulmonary VSD or ventricular septal defect. The orifice of fetal aorta is placed away from the left ventricle and hence has poor prognosis compared to a sub aortic VSD. This anomaly is a variant of DORV and called Taussig Bing variant. STIC ultrasound images of DORV with Taussig Bing anomaly (STIC or 4D color Doppler ultrasound of fetal heart) are courtesy of Dr. Firoz Bhuvar, MD.
dilated-cardiomyopathy-in-fetus
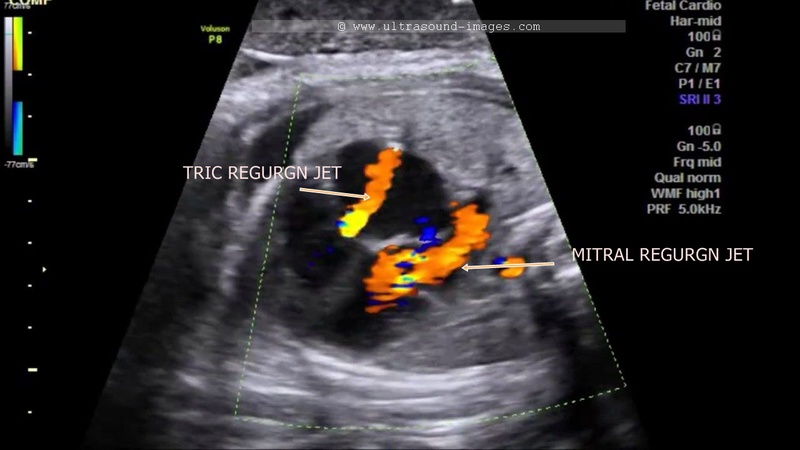

This third trimester fetus shows generalised or global enlargement of the heart including both fetal ventricles as well as the fetal atria. The fetal echocardiography video also shows both tricuspid as well as mitral regurgitation although both appear to be mild in nature. These ultrasound findings suggest this to be a case of dilated cardiomyopathy. Dilated cardiomyopathy is usually the result of intrauterine infections such as toxoplasmosis and cytomegalovirus infections. In this patient, there was a history of analgesic intake by the mother during the pregnancy which may have resulted in the pathology in this fetal heart. Dilated cardiomyopathy typically reveals dilation of one or more chambers of the heart with usually associated mild or severe mitral and/ or tricuspid regurgitation. Conservative treatment is usually sufficient to control or even reverse all these ultrasound findings. Another finding which may be present in cases of dilated cardiomyopathy is echogenic intracardiac foci. this ultrasound video and images of dilated cardiomyopathy are courtesy of Firoz Bhuvar, MD.
References:
ultrasound imaging of dilated cardiomyopathy in fetus (article in American heart Association Journal)
ARSA-aberrant-right-subclavian-artery
Aberrant right subclavian artery or ARSA as it is commonly known, is one of the commonest anatomical variants of the aortic arch. Some authors consider this to be a congenital anomaly; however, current medical literature classifies this as nothing more than a normal variant. Aberrant right subclavian artery is characterized by the origin of the right subclavian artery from the distal part of the aortic arch which passes to the right arm, posterior to the esophagus and trachea. The diagnosis of aberrant right subclavian artery (ARSA) is hence not very difficult, even during the second trimester of pregnancy. Using colour Doppler ultrasound, it is possible to see the course of the aberrant right subclavian artery as it passes posterior to the trachea and the esophagus in the fetus. The colour Doppler ultrasound video below (courtesy of Firoz Bhuvar, MD), demonstrates the aberrant right subclavian artery , which is visualized on appropriate low PRF settings on colour Doppler study. The only important differential diagnosis in cases of ARSA, is the azygos vein , which also appears similar, but can be distinguished by the entry of the azygos vein into the superior vena cava. Also, special Doppler ultrasound as seen in the video clearly shows arterial flow waveform in cases of aberrant right subclavian artery. The best sonographic view to image this vessel is the three vessel trachea view.
This is a relatively common ultrasound finding during fetal ultrasound with an incidence of almost 1.5% of the entire population. One notable point to be remembered is that there is a high incidence of trisomy 21 associated with aberrant right subclavian artery. If other cardiac anomalies are seen, there is a danger of other chromosomal aneuploidies.
References: Journal of ultrasound article on aberrant right subclavian artery
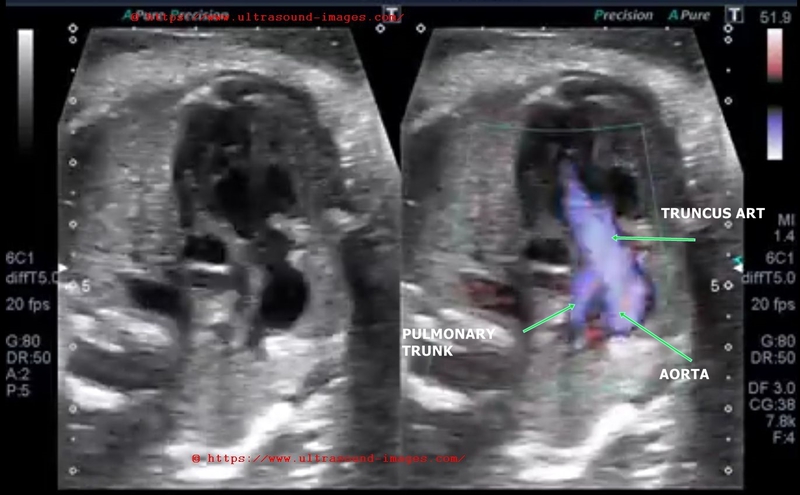
truncus-arteriosus-fetal-echo-STIC
 STIC ultrasound fetal echo truncus arteriosus
STIC ultrasound fetal echo truncus arteriosus
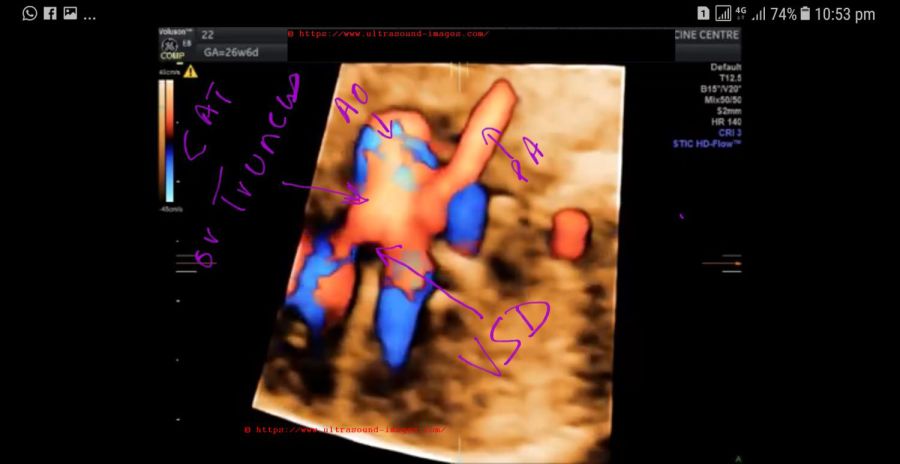
Case-1: (above) STIC fetal echo and 3D/4D color Doppler ultrasound video and image above show the following:
- large common arterial trunk or CAT emerging from above both ventricles with a large VSD (ventricular septal defect).
- By Collette and Edwards classification of truncus arteriosus or CAT (common arterial trunk) this is a type 1 truncus arteriosus/ CAT anomaly. Here the truncus gives rise to a large aorta and a common pulmonary trunk
- In type 2- two separate pulmonary arteries emerge from the truncus arteriosus but are proximal to each other
- In type-3- the right and left pulmonary arteries are widely separate as they emerge from the truncus or CAT
- CAT or truncus arteriosus forms about 1% of all congenital cardiac anomalies and is thus a very rare cardiac malformation.
- asscociated with 22q11 microdeletion chromosomal anomaly
- other congenital malformations may be present.
- The STIC 3D/4D color Doppler ultrasound video (fetal echocardiography) above of truncus arteriosus (CAT- common arterial trunk) in a late 2nd trimester fetus is courtesy of Dr. Firoz Bhuvar, MD, India.
Reference: STIC sonography and 3D/4D echo of truncus arteriosus or CAT
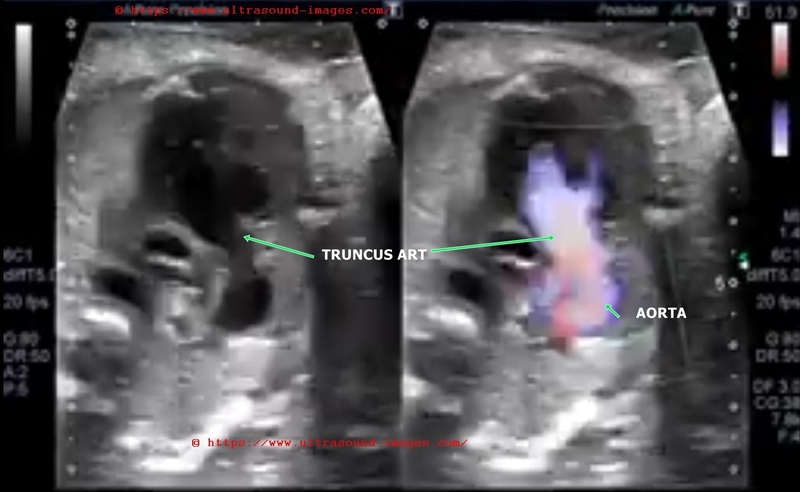
Case-2: (see below) color Doppler ultrasound video and fetal echo of truncus arteriosus or CAT:
- in this case too there is a large VSD (ventriculo-septal defect) with the truncus arteriosus over riding the defect in the ventricular septum.
- The truncus receives blood from both ventricles right and left
- The aorta and pulmonary trunk are seen emerging from the truncus.
Case-2 fetal echo of truncus arteriosus or CAT is courtesy of Dr. Vishal Kumat
VSD-STIC-ultrasound
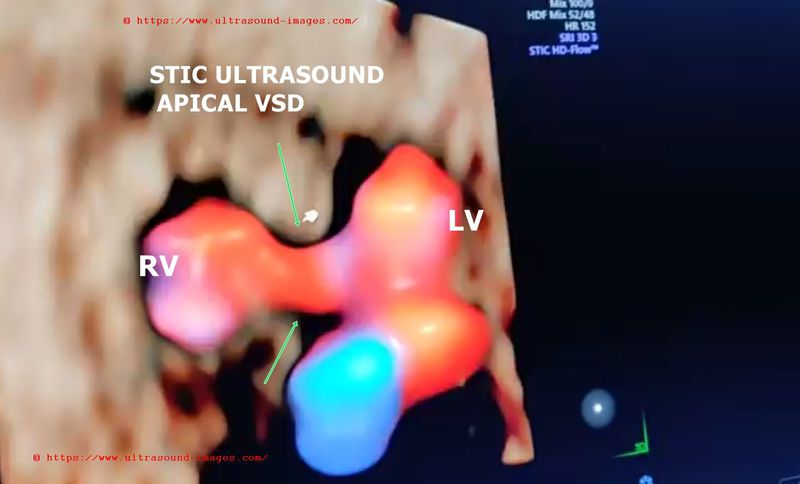
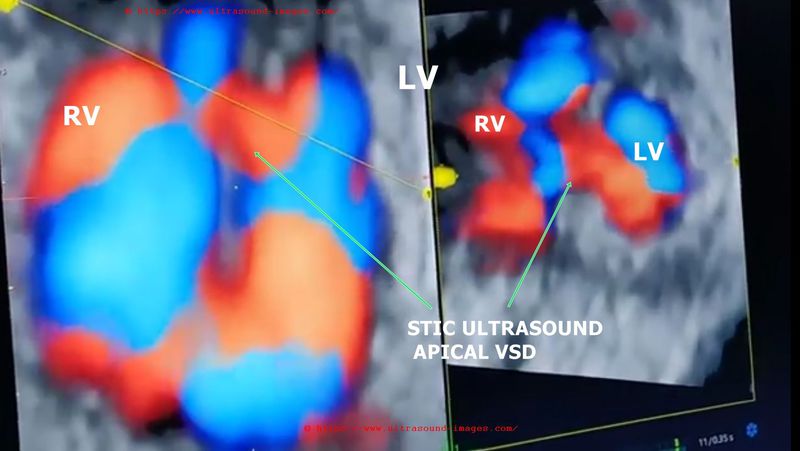
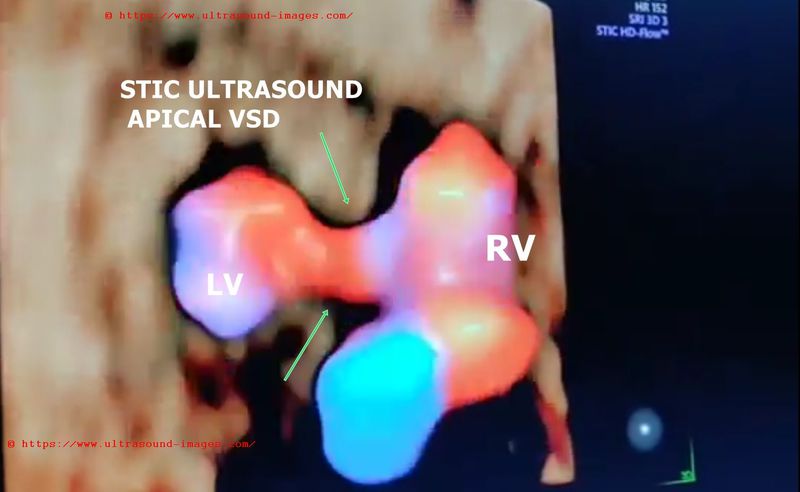
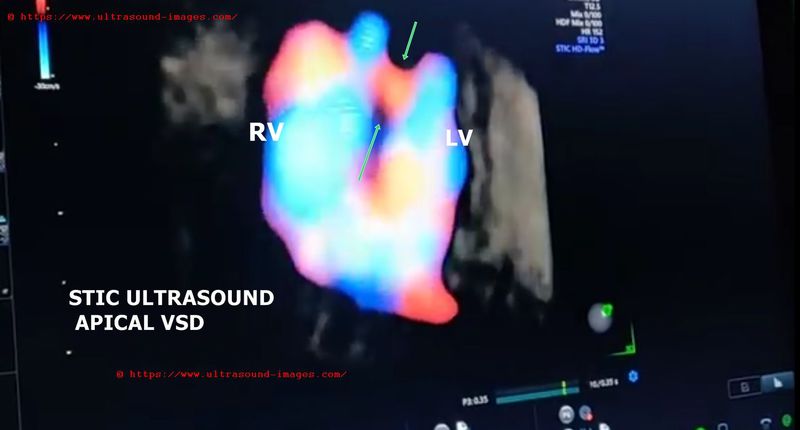
21 weeks fetus shows a small apical VSD or ventricular septal defect
= size of VSD defect is less than 3mm
= small apical VSD is known to close spontaenously during infancy
= hence good prognosis in this case
= here the VSD defect is seen best as color flow signal across the ventricular septum near apex
= the VSD defect in the fetal heart itself is poorly seen on B-mode ultrasound. However, STIC 4D ultrasound shows (see the video above) flow across the miniscule defect in the ventricular septum near the apex.
= apical VSD are comparatively rare and it is more common in the middle muscular septum or membranous region of the ventricular septum.
(Video and STIC ultrasound images of apical VSD in fetus courtesy of Dr. Jagrut Joshi, MD) (edits: by Dr. Joe Antony, MD)
References: STIC sonography of VSD and its prognosis
atrial-septal-aneurysm

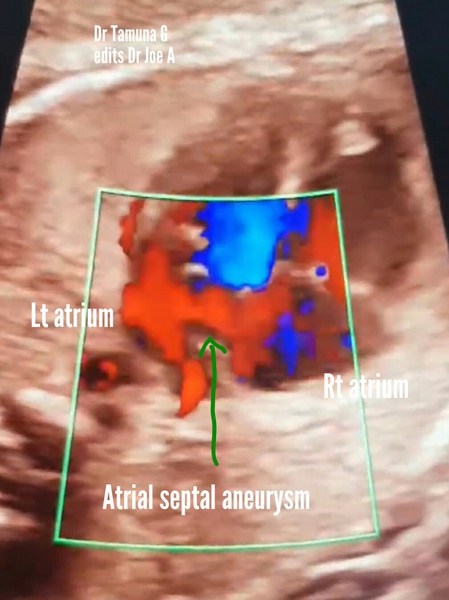
This 30 week fetus fetal heart echocardiography (echo) video and images show:
= atrial septal aneurysm with bulging of the membrane covering the foramen ovale (a part of the septum primum of the interatrial septum)
= the membrane of the septum primum bulges from the interatrial septum into the left atrium due to pressure from the blood flowing from the right atrium across the foramen ovale
=diagnostic point: to be labelled atrial septal aneurysm- the membrane should bulge more than 50 % of the width of the left atrium
= other synonyms for atrial septal aneurysm: foramen ovale aneurysm, aneurysm of septum primum
= fetal left atrium is smaller than normal due to obstruction to flow (by atrial septal aneurysm) from Rt. atrium across foramen ovale.
= delayed complications include: cardiac arrythmias
= usually not associated with other cardiac anomalies
= atrial septal aneurysm usually disappears after boirth due to closure of the foramen ovale.
= the fetal ultrasound echo video of atrial septal aneurysm and images are courtesy of Dr. Tamuna G (edits by me, Dr. Joe A)
References: Ultrasound echo imaging of atrial septal aneurysm
© 2026, Joe Antony, MD All images and content in this site are copyrighted. www.ultrasound-images.com When visiting this site, we may use cookies to improve the performance of this site. Use of this site means you accept the use of cookies. Read our privacy policy at this page: https://www.ultrasound-images.com/privacy-policy/