
Ultrasound images of fetal Brain
Contents of this page
- Dandy-Walker malformation
- Aneurysm of Vein of Galen
- Acrania
- Choroid plexus cyst
- Occipital meningocele with encephalocele
- Aqueductal stenosis causing obstructive hydrocephalus
- Choroid Plexus papilloma in fetus
- intraventricular adhesions in fetus
- fetal epidermal cyst of the scalp
- mega-cisterna-magna
- Anencephaly-in-fetus
- Anencephaly-3D-ultrasound
Dandy-Walker malformation



Sonography in Dandy-Walker syndrome:
The above ultrasound images of fetal brain show hypoplastic cerebellum and absent vermis with enlarged 4th ventricle which is typical of Dandy-Walker malformation. Images courtesy of Dr. Gidda Ramaiah, India. (Note: click to view larger images).
Reference:
1) http://www.emedicine.com/radio/topic206.htm (free)
2) Herniated Dandy-Walker cysts, Prenatal Diagnosis (free article)
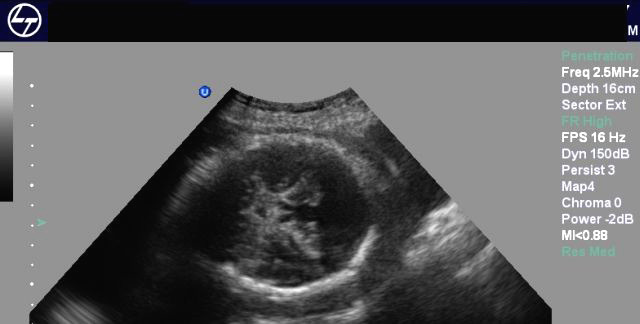
Aneurysm of Vein of Galen
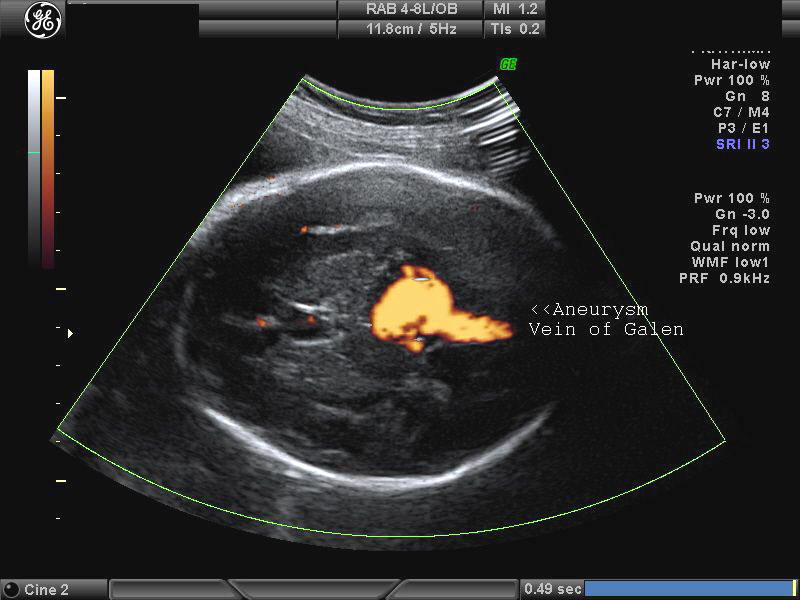

Ultrasound images of intracranial venous aneurysm in fetus:
These are ultrasound images of a 30 week old fetus. Sonography of the fetal brain reveals an anechoic (cystic) lesion posterior to the thalamus and the midbrain. Color doppler image reveals significant flow within this lesion. These ultrasound images are diagnostic of aneurysm of the Vein of Galen. Vein of Galen aneurysms are usually diagnosed in the 3rd trimester. They are usually produced by draining of multiple arteriovenous malformations in the adjacent part of the fetal brain. Differential diagnosis of such lesions includes arachnoid cysts, porencephalic cysts choroid plexus cysts and choroid plexus papilloma (easily diagnosed using color doppler imaging). Choroid papillomas are solid lesions unlike the cystic nature of a vein of Galen aneurymsmal malformation. The other cystic lesions mentioned above would not show flow signal within the lesion on color or Power Doppler imaging.
References:
1) sonoworld article on vein of Galen aneurysm
2)AJNR article on vein of Galen aneurysmal malformation
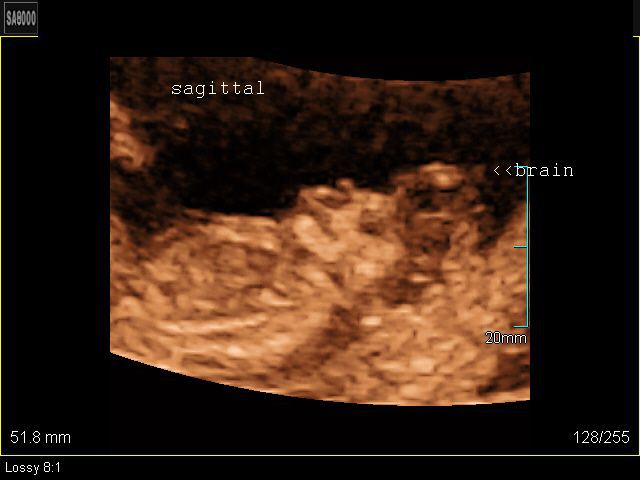
Acrania




Download my E book for Amazon Kindle (download free Kindle reader for i Phone or Android)
Assorted ultrasound cases- by Joe Antony, MD
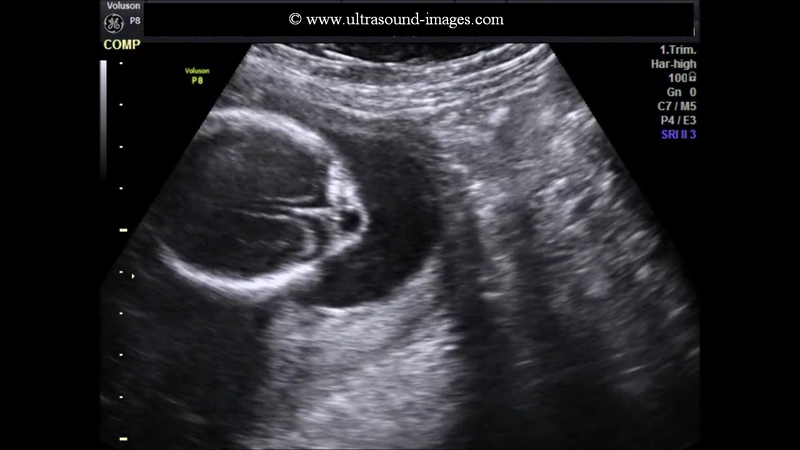
This 12 week fetus shows prolapse of the brain outside the cranial cavity with absence of the cranial vault (calvarium). The brain is almost normal in size for the gestational age of this fetus. These ultrasound images are diagnostic of acrania. This has to be distinguished from anencephaly, where the brain is absent or grossly atrophic. The colored pictures show 3D ultrasound images of the fetus. Images taken using a Medison SA 8000, color doppler and 3D ultrasound machine, courtesy of Dr. Arun Mahajan, Delhi, India.
Another case of acrania (GE P5 ultrasound system), on transvaginal ultrasound in a 11 weeks 5 days fetus:
Reference: http://www.thefetus.net/page.php?id=77 (free article and images)
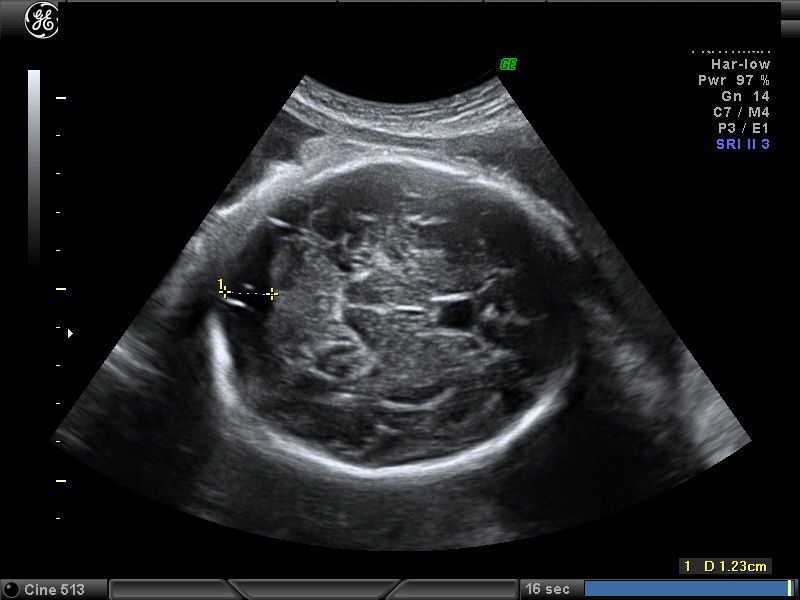
Choroid plexus cyst


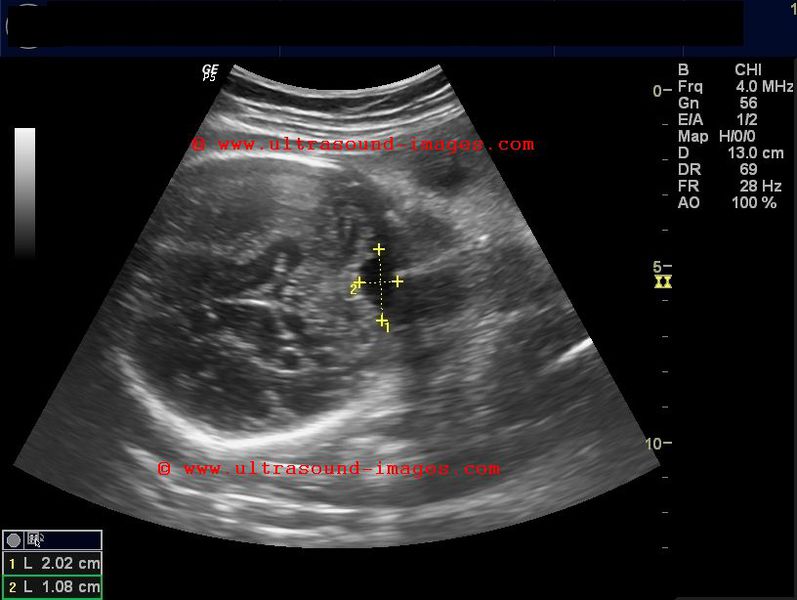
Sonography of the fetal brain revealed a cystic lesion of 9 mm., in the choroid plexus of the left lateral ventricle. These ultrasound images suggest choroid plexus cyst. Images taken using a Nemio-XG color doppler machine. Clinically, isolated choroid plexus cysts without the presence of associated fetal anomalies have little significance (see link below) and are known to resolve spontaneously.
Reference:
1) significance of choroid plexus cysts (free article- rated excellent).
2) Choroid plexus cysts and Trisomy 21 (free abstract)
Occipital meningocele with encephalocele



Sonography of the fetal head showed-a) a small skin covered herniation of meninges through a small defect in the occipital region of the skull. b) presence of part of brain tissue in the herniated sac. The 3rd image shows the sac floating in the amniotic fluid. These ultrasound images suggest a diagnosis of occipital meningocele with encephalocele.
Images courtesy of Gunjan Puri, MD, Surat, India. He used a Toshiba Xario machine for these images.
Reference: http://drjoea.googlepages.com/obstetric-3 (visit this page for free ultrasound images and links for this fetal anomaly)
Aqueductal stenosis causing obstructive hydrocephalus
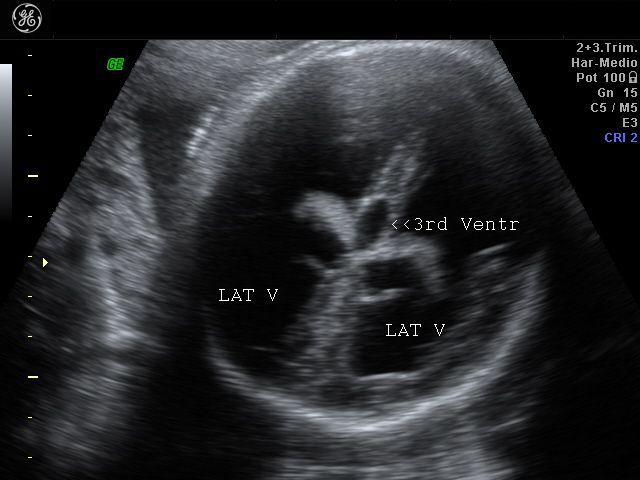

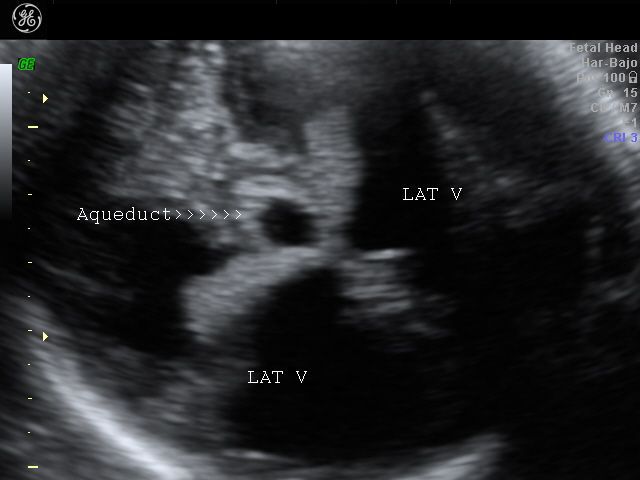
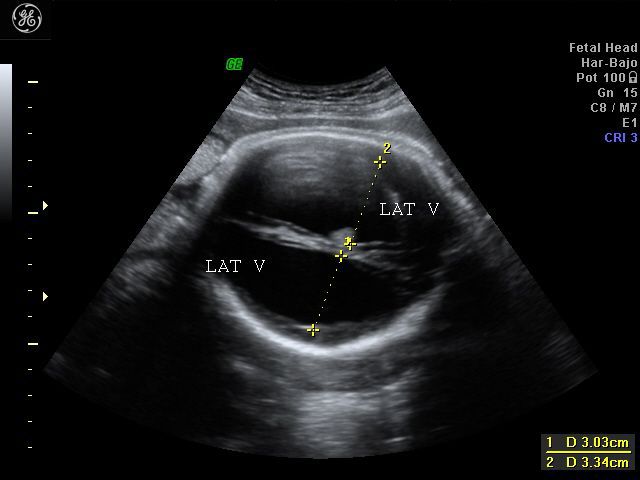
Sonography of the fetal brain done on this 3rd trimester fetus shows marked dilatation of the lateral ventricles bilaterally. The 3rd ventricle and upper part of the cerebral aqueduct or aqueduct of Sylvius are also dilated. The choroid plexus on both sides (within the lateral ventricles) appear to "dangle" or droop to the dependent part of the brain. The lateral ventricles measure more than 30 mm. (3 cms.) on both sides at the level of the atria. The cerebral hemispheres show marked thinning of the cerebral tissue (both cortex and white matter), but are visualized as thin tissue along the cranial vault. Current literature holds that any fetal lateral ventricular measurement of more than 10 mm. (at the atria) is pathological. These ultrasound images suggest a diagnosis of aqueductal stenosis with intraventricular obstructive hydrocephalus. (Ultrasound images taken with GE Voluson machine are courtesy of Dr. Martin Horenstein, MD, Argentina).
The main criteria used to diagnose hydrocephalus/ ventriculomegaly are: 1) atrial size (greater than 10 mm.) 2) Ventricle to cerebral hemisphere ratio ( normal ranging from 74 % at 16 weeks to 35 % by 25 weeks). 3) The combined anterior horn width (normal = less than 20 mm.)
I have a short ultrasound video clip of aqueductal stenosis posted here:
http://cochinblogs.blogspot.com/2009/08/hydrocephalus-in-fetus-aqueductal.html
Reference: http://emedicine.medscape.com/article/1135286-overview
Choroid Plexus papilloma in fetus
Ultrasound image choroid papilloma

Color Doppler image choroid plexus papilloma

MRI scan image- fetal choroid papilloma


This fetus showed a large, lobulated echogenic mass filling almost the entire right lateral ventricle (see ultrasound image top row -Left). The color Doppler image shows the mass containing a few small vessels feeding it. The lateral ventricles on both sides do not show significant dilatation. However, the MRI scan image of the fetal brain (bottom) shows significant midline shift and mass effect on the fetal brain. Such an echogenic lesion in the lateral venrticle is typical of mainly two kinds of lesions- choroid papilloma and intracranial hematoma. The presence of vessels within the mass is suggestive of a neoplasm. In this case the diagnosis based on post delivery histopathology is - choroid plexus papilloma of the right lateral ventricle. The absence of hydrocephalus is typical of choroid plexus papillomas that fill the ventricle until it has enlarged further and caused compression of the outflow of CSF from the ventricular system.
References: http://www.sonoworld.com/
http://emedicine.medscape.com/
Intraventricular adhesions in fetus


This early third trimester foetus shows multiple septations within both lateral ventricles (see the ultrasound images of the fetal brain shown above). Arrows point to the septations, or to be more precise, adhesions within both lateral ventricles of the fetus. In addition, there is evidence of increased echogenicity of the peri-ventricular regions, suggesting the possibility of cytomegalovirus (CMV) infection. Cytomegalovirus infection is known to produce multiple such lesions within the fetal brain, including, sulcal and gyral anomalies, intraventricular adhesions, ventriculomegaly and subependymal cystic lesions within the lateral ventricles of the fetal brain.
These ultrasound images of fetal intraventricular adhesions are courtesy of Firoz Bhuvar, MD.
References:
sonographic features of cytomegalovirus infection in fetal brain
ultrasound imaging of intraventricular adhesions in fetus and neonate
Fetal epidermal cyst of the scalp


This second trimester fetus shows a cystic lesion although small in the occipital region. This should send alarm bells ringing in the direction of the possibility of a major congenital anomaly of the fetus such as an occipital encephalocle or meningocele. Such a diagnosis can significantly alter the management of the case. However, in this fetus, the diagnosis based on the ultrasound images above, is that of an epidermal cyst in the occipital region. A diagnosis of encephalocele can be ruled out as there is no evidence of breach in the continuity of the occipital bone, as well as the absence of intracranial brain pathology, normal shape of the fetal skull and a normal ventricular system of the fetal brain. Thus this cystic lesion appears to be confined to the fetal scalp and the ultrasound images above point to a diagnosis of fetal scalp cyst- in this case epidermal cyst. These B mode and 3D ultrasound images of fetal scalp cyst are courtesy of Firoz Bhuvar, MD.
References:
1. Sonography of fetal epidermal scalp cyst- Journal of ultrasound
2. Ultrasound imaging of fetal epidermal scalp cyst- sonoworld
Mega-cisterna-magna
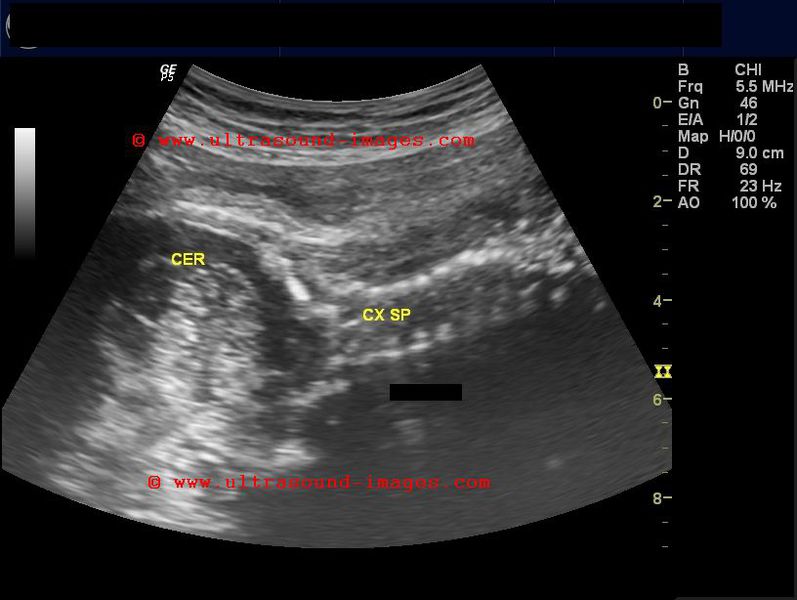
The cisterna magna is the CSF containing space posterior to and surrounding the cerebellum in the posterior fossa. The normal anteroposterior width of the cisterna magna in third trimester of pregnancy in the fetus is less than 10 mm, as measured from the posterior surface of the vermis of the cerebellum to the anterior surface of the occipital bone in the axial plane of the fetal head. When this space is widened and greater than 10 mm, a number of diagnostic possibilities arise, including Dandy Walker malformation, Blakes pouch cyst, arachnoid cyst and mega cisterna magna. In this fetus (see ultrasound images above), the size of the fetal head is normal , as are the lateral ventricles. However, the anteroposterior width of the cisterna magna is greater than 10 mm ( here it measures 12 mm) in the axial plane. In addition, the fetal cerebellum and the vermis of the cerebellun are well preserved and normal in size and shape. the fetal fourth ventricle is also normal in size and the cisterna magna freely communicates with the surrounding sub arachnoid spaces. In addition, the posterior fossa does not here to be enlarged. All these ultrasound findings point to a diagnosis of mega cisterna magna in this fetus.
In this case study of mega cisterna magna, we have obtained ultrasound images in multiple planes of the fetal head and brain. It is important to measure the width of the cisterna magna in the correct axial plane to obtain the anteroposterior space between the vermis of the cerebellum and the anterior surface of the occipital bone. In addition, a mid-sagittal section of the posterior fossa is also mandatory to rule out any defect or malformation of vermis of the cerebellum. often it may be difficult to do multi-axial plane sonographlc study of the posterior fossa on B-mode ultrasound. In such cases, multiplanar imaging using 3-D ultrasound is very helpful. (In this case, the images are shown below).
References:
Sonographlc imaging of mega cisterna magna- Journal of ultrasound

Anencephaly-in-fetus
Fetal anencepahly is a neural tube defect characterized by near total absence of cerebral cortical tissue (the cerebral hemispheres) though parts of the barin stem may be present. In addition, the fetal calvarium is invariably absent. The fetal orbits and eyeballs protrude or bulge resulting in a "frog eye" apperance. Polyhydramnios is usually present due to poor swallowing of fluid. This B mode ultrasound image (above) shows a classic fetal anencephaly (image courtesy of Dr. Jorge Hernandez).
Reference: http://radiopaedia.org/articles/anencephaly
Anencephaly-3D-ultrasound



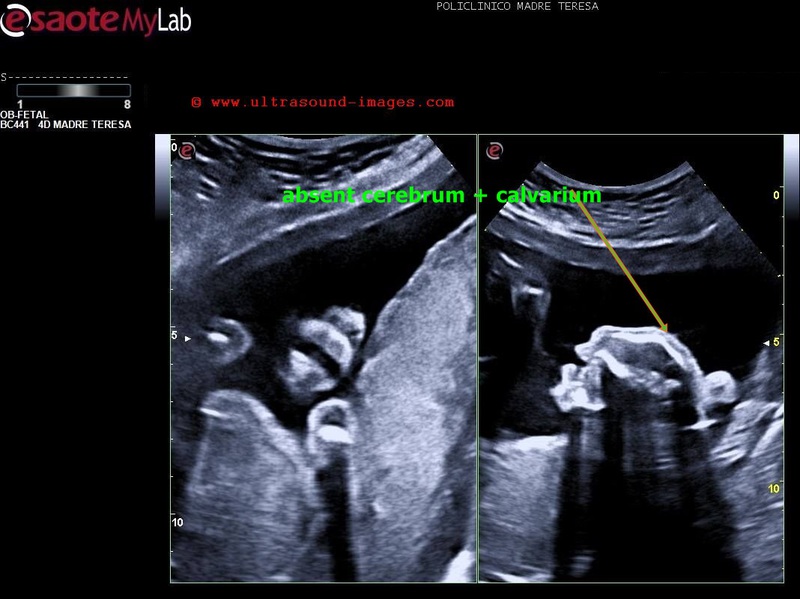
These 3D ultrasound images by Dr. Firoz Bhuvar, MD, show clearly the extent of the absence of calvarium and cerebral hemispheres in this fetus. Clearly diagnostic of anencephaly. The frog eye sign is clearly visible in these images of anencephaly. the prognosis is very poor and termination of pregnancy is imperative.
© 2026, Joe Antony, MD All images and content in this site are copyrighted. www.ultrasound-images.com When visiting this site, we may use cookies to improve the performance of this site. Use of this site means you accept the use of cookies. Read our privacy policy at this page: https://www.ultrasound-images.com/privacy-policy/