
scrotum
Contents of this page
- Epididymitis
- Testicular microcalcification/ microlithiasis
- Microliths of testis in newborn
- Testicular mass- germ cell tumours- seminoma
- Case-2: Malignant mass of the testes
- Hydrocele- B-mode grey scale and 3-D images
- Multiple epididymal cysts
- Case-2: Multiple epididymal cysts- 3D ultrasound images
- Spermatocele
- Varicocele: (dilatation of veins of Pampiniform plexus of scrotum)
- Bilobed testes: (Bilobed testicles/ bilobed testis)
- Simple cyst of testes
- Cryptorchidism
- Ultrasound images of abdominal testis
- Retractile testis
- Tubular ectasia of rete testes
- Atrophy of testis
- AVM of testis (intratesticular arteriovenous malformation)
- Orchiopexy (orchidopexy)
- Indirect inguinal hernia forming large Right scrotal swelling
- Epidermoid cyst of testis
- hydrocele with display of spermatic cord
- filarial-dance-scrotal
- macro-calcification-testis
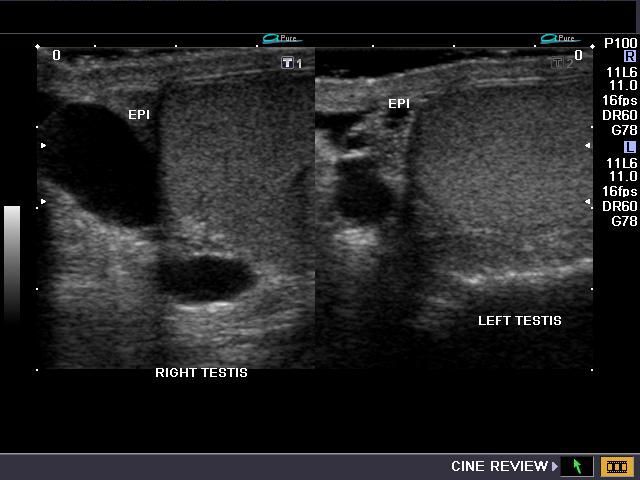
Epididymitis
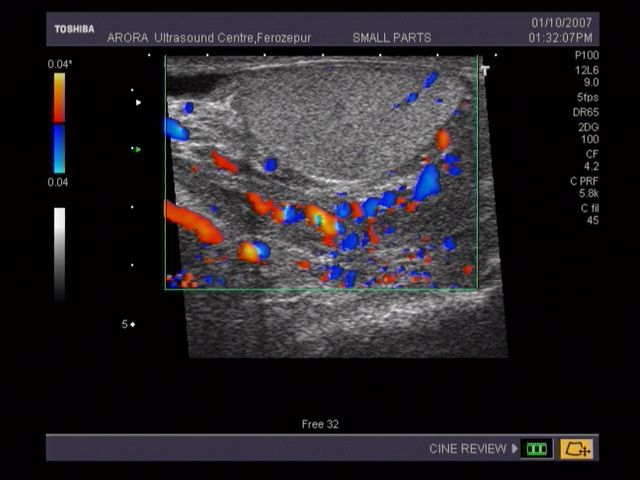


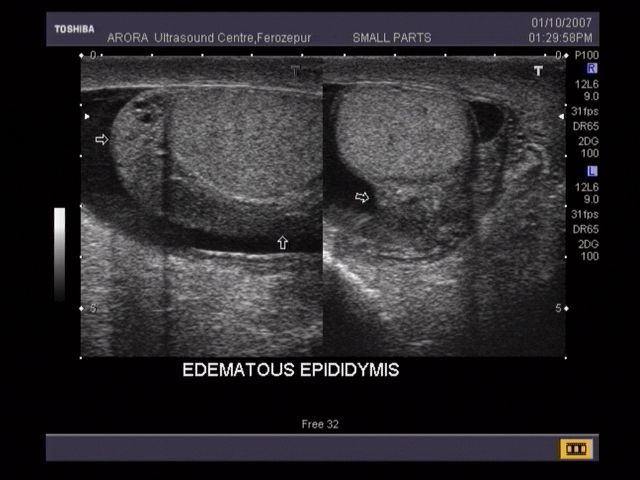
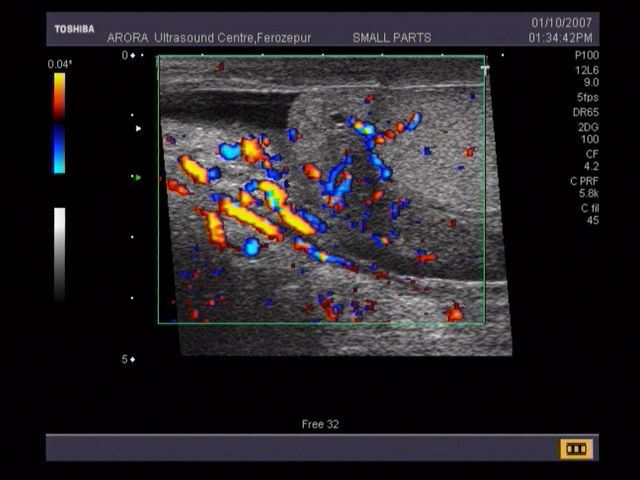
This male patient complained of pain in the scrotum. B-mode ultrasound images reveal a swollen and edematous epididymis. The entire structure including the head, body and tail of the epididymis appear to be involved. Color doppler images confirm the presence of inflammation by the increased vascularity. Surprisingly, the testes itself appears to be spared. These ultrasound images are diagnostic of epididymitis. Images courtesy of Dr. Vikas Arora, Ferozepur, India.
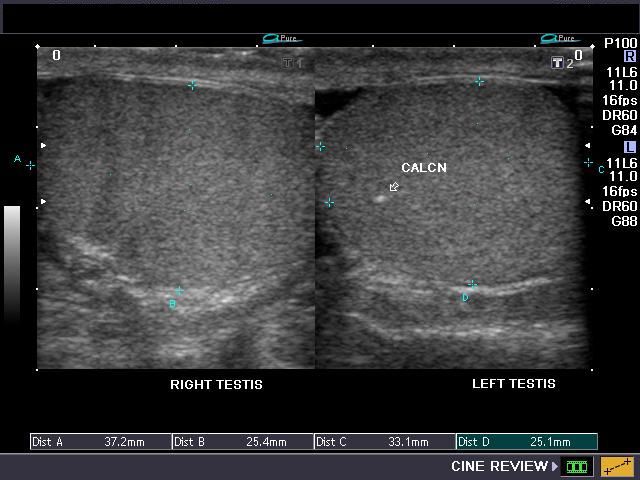
Testicular microcalcification/ microlithiasis
Case-1:

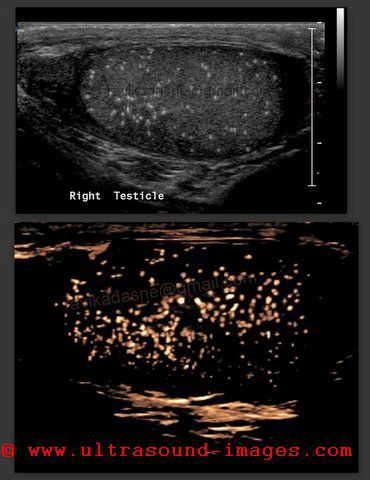
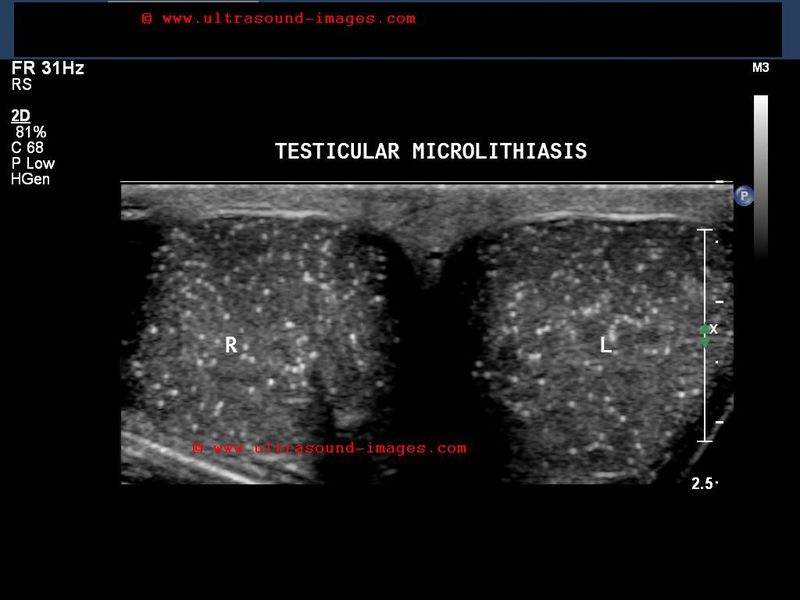

The above ultrasound images (from 3 different patients) show a) more than 5 calcific foci per ultrasound image of the testes b) sizes of the calcification is in the range 1 to 3mm. 3) bilateral involvement. These ultrasound images are diagnostic of testicular microlithiasis. Microlithiasis of testes is associated with higher incidence of intratubular germ cell neoplasia of testes and other tumors of this organ. Images courtesy of Dr. Ravi Kadasne (case 1) and Shlomo Gobi (case 2). 3D ultrasound study (courtesy Dr Ravi Kadasne) of the testicular microliths is also seen (image top, middle) showing a starry night appearance.
Reference:
1)Free article on Testicular microlithiasis (AJR) (free article and images)- excellent
2) http://www.ispub.com/ostia/index.php?xmlFilePath=journals/iju/vol3n2/testicular.xml(free)



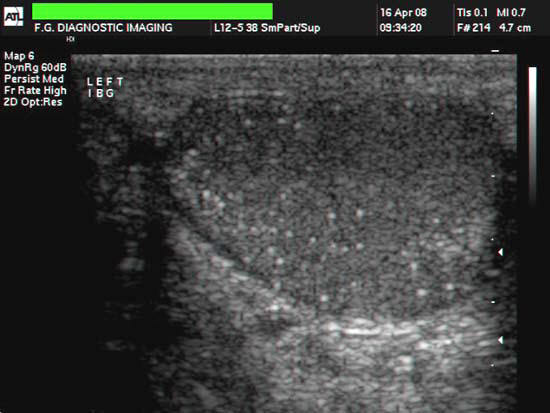
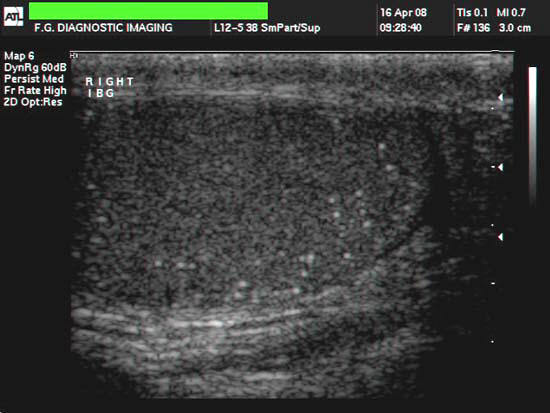
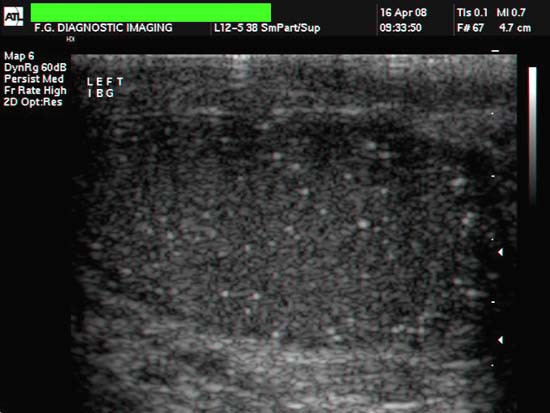
The above ulltrasound images and Color Doppler image show testicular microliths (left testis) in a new born baby. Testicular calcifications can occur in any age group; however the occurrence of this condition in a newborn is very rare. The color Doppler study showed normal vascularity in the affected testis. Such cases need to be followed up for changes such as germ cell tumor and more benign conditions such as epididymitis, orchitis and varicocele as well as testicular atrophy. Studies show possible link between Testicular microlithiasis in infants and Down's syndrome. Ultrasound images are courtesy of Mr. Shlomo Gobi, sonographer, Israel.
Reference: http://www.pedrad.info/?search=20030222173416&lang=en#a1
Testicular mass- germ cell tumours- seminoma

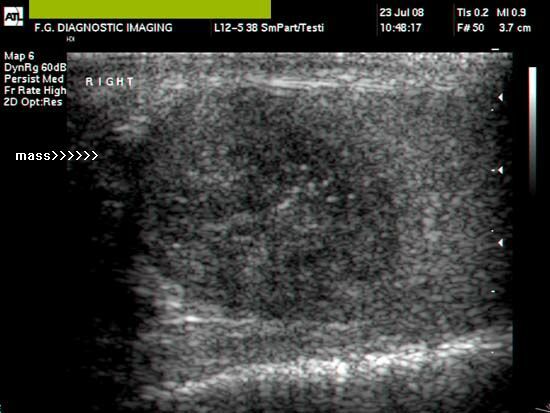


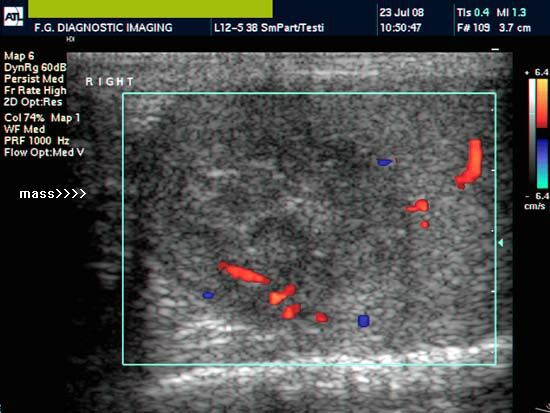

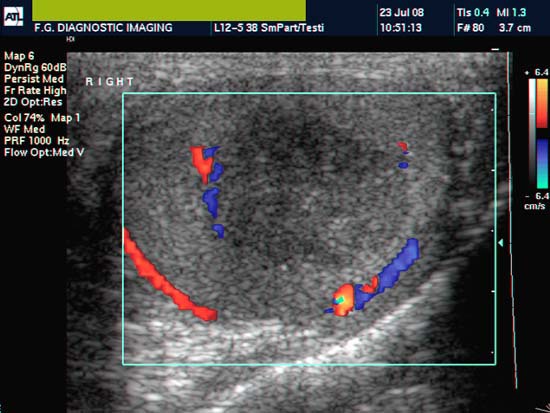
This young male adult patient had a swelling in the right testicle which was confirmed on palpation. Sonography of the testes revealed: 1) microcalcification in the otherwise normal left testes and also in the affected right testes. 2) A large mass (about 2 cms. in size) in the upper pole of right testes. Mass is markedly hypoechoic and inhomogenous with irregular, poorly defined margins. 3) On color doppler imaging, the mass shows increased vascularity and feeding vessels. These ultrasound images suggest a diagnosis of Germ cell tumour of the right testes, probably a seminoma. Ultrasound and color doppler images courtesy of Shlomo Gobi, Israel. The machine used here is an ATL- Philips HDI 3000.
Reference:
1)http://www.emedicine.com/Med/topic2250.htm(free article)
2)testicular seminoma ultrasound : Danilo Sirigu, MD (images and video)
3)Unilateral testicular microlithiasis associated with a seminoma (free abstract).This article describes the significance of testicualr microlithiasis as an associated finding in testicular masses.
Case-2: Malignant mass of the testes
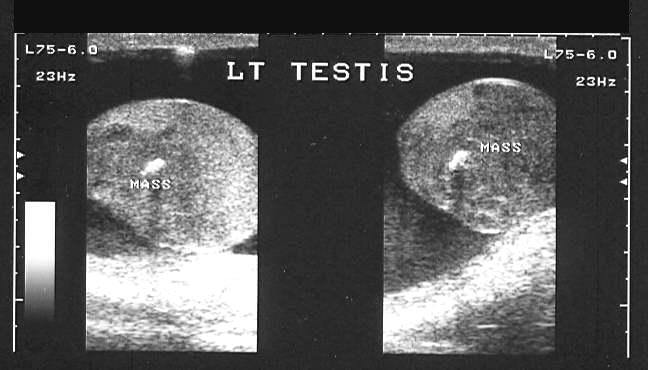

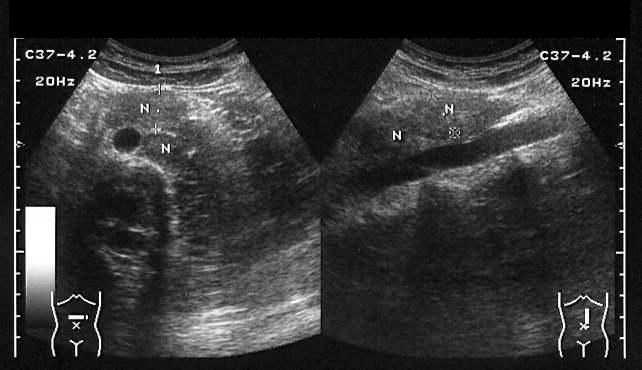
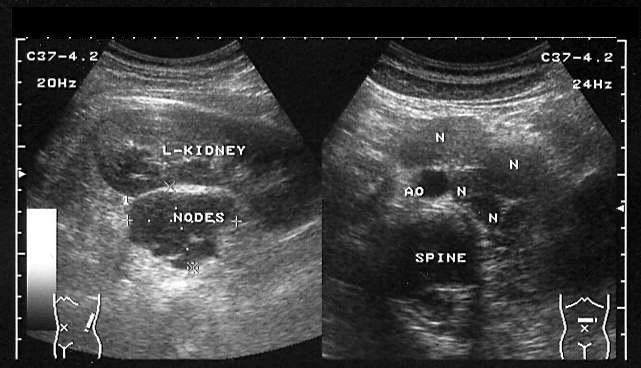

This male patient presented with left testicular mass and pain. Ultrasound images of the left testis show a large hypoechoic mass of the left testis with increased vascularity of the lesion on color Doppler imaging. Ultrasound images of the retroperitoneal region show multiple enlarged lymph nodes, near the left kidney and para-aortic regions. X-ray of the chest shows multiple radiopaque coin lesions throughout both lung fields s/o metastases. These findings suggest malignant mass, possibly seminoma (or other germ cell tumor) of the left testis. All ultrasound pictures of testicular cancer are courtesy of Dr. Ravi Kadasne, MD, UAE.
Hydrocele- B-mode grey scale and 3-D images

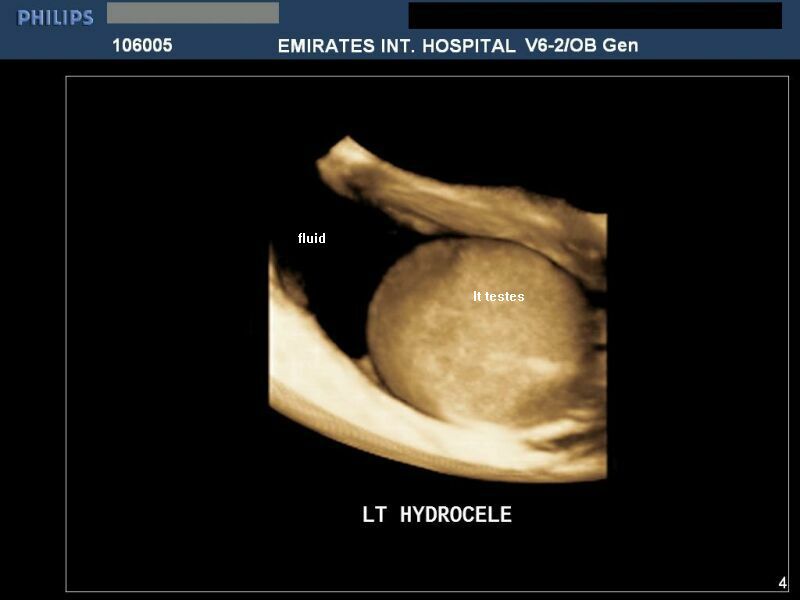
Hydrocele is the pathological collection of fluid within the tunica vaginalis of the scrotum. Here, the serous fluid collection is seen within the tunica vaginalis around the left testes. Observe the detail seen in the 3-D (or 3 dimensional) ultrasound image on the right side. 3-D ultrasound image of hydrocele, courtesy of Dr. Ravi Kadasne, MD, UAE, who used a Philips IU 22 machine for it.
Reference:
1)http://drjoea.googlepages.com/gallery-testes(free article and images).
2)http://drjoea.googlepages.com/scrotum (free ultrasound images and articles).
3) See this link too:http://www.squidoo.com/scrotum a nice page on scrotal swellings and the role of sonography.
Multiple epididymal cysts




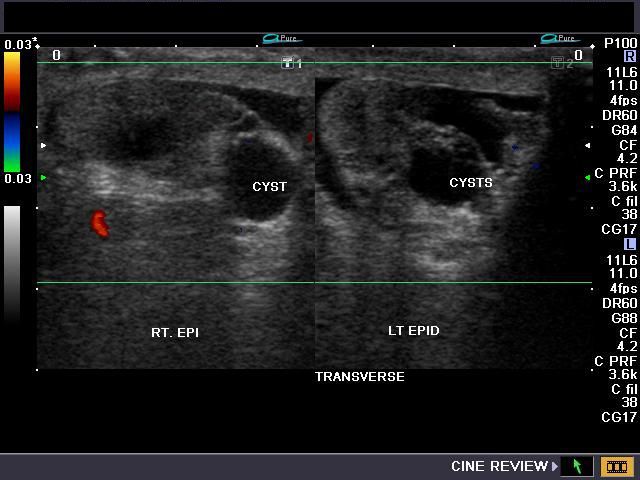
This middle aged male patient presented with symptoms of nodular swelling of the scrotum. On sonography, there were multiple cystic lesions of 1 to 1.6 cms. in the region of the heads of epididymis bilaterally. Color and Power Doppler images show no flow within the cystic lesions. These ultrasound images are diagnostic of multiple cysts of the head of the epididymis. Epididymal cysts are usually asymptomatic unless large or multiple and may be seen following vasectomy. There are also solitary calcific lesions in the testes (which do not appear to be of clinical significance). These ultrasound images were taken using a Toshiba Nemio- XG ultrasound machine.
Reference: http://www.mypacs.net/cases/EPIDIDYMAL-CYST-20141.html
Case-2: Multiple epididymal cysts- 3D ultrasound images

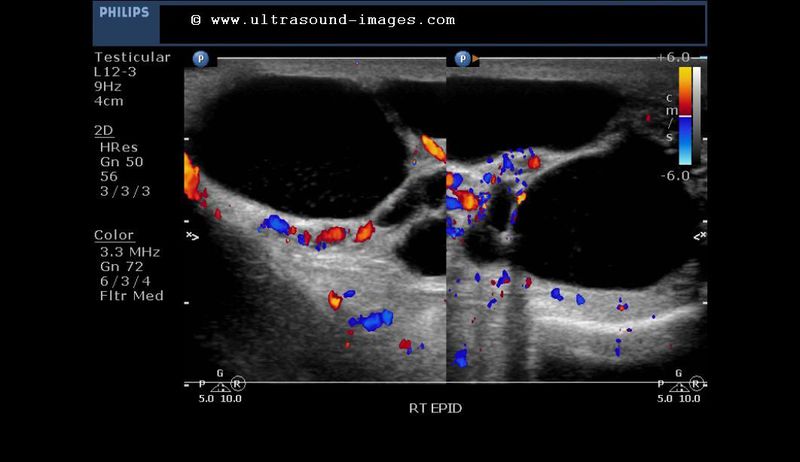
Shown above are 2D B-mode and color Doppler ultrasound images of multiple right epididymal cysts in the head of the right epididymis. Surprisingly the septae show remarkable vascularity
3D ultrasound images (longitudinal section) of the epididymal cysts




Observe the fine internal details of the cysts and the nature of the walls of the epididymal cysts in these 3D ultrasound images of the lesions.
Spermatocele


This patient had history of a painless nodule at the upper pole of the right testis since 2 years. Ultrasound images of the scrotum show a rounded cystic lesion with abundant echogenic particulate matter within it. The cyst is located in close relation to the head of right epididymis. These ultrasound findings suggest a diagnosis of spermatocele involving the head of right epididymis. Spermatoceles are formed by obstruction of the fine ducts within the epididymis or spermatic passages, resulting in outpouching or diverticuli formation with sperm containing fluid collecting within the cystic lesion. It is often the presence of debris within the cyst that distinguishes spermatoceles from simple cyst of the epididymis. Power or Color Doppler imaging sometimes shows movement of the debris within the cyst.
Reference:http://www.jultrasoundmed.org/cgi/reprint/27/1/141.pdf
Varicocele: (dilatation of veins of Pampiniform plexus of scrotum)
A) Exratesticular varicocele

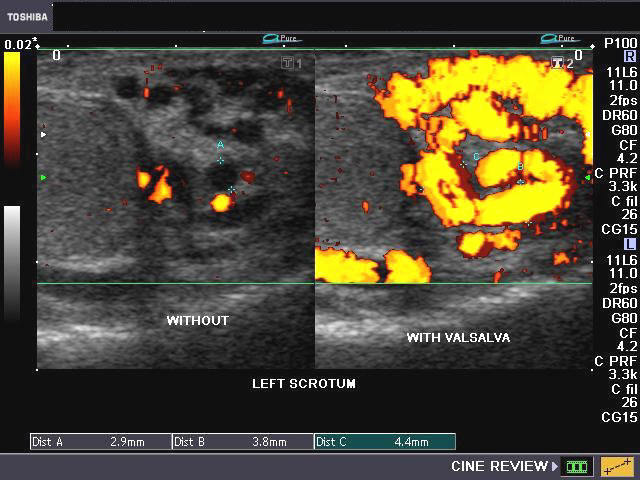
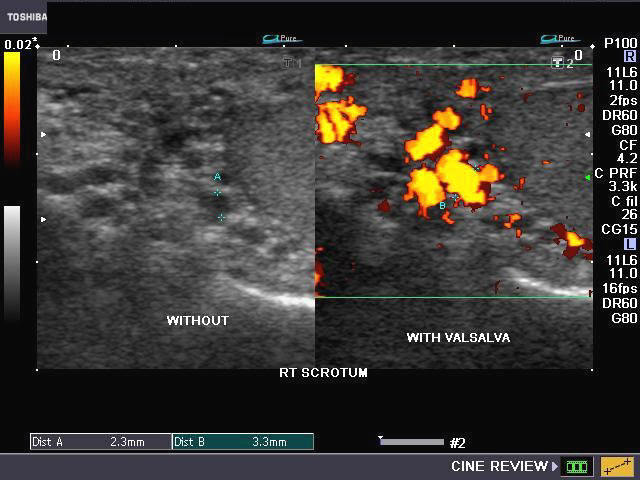

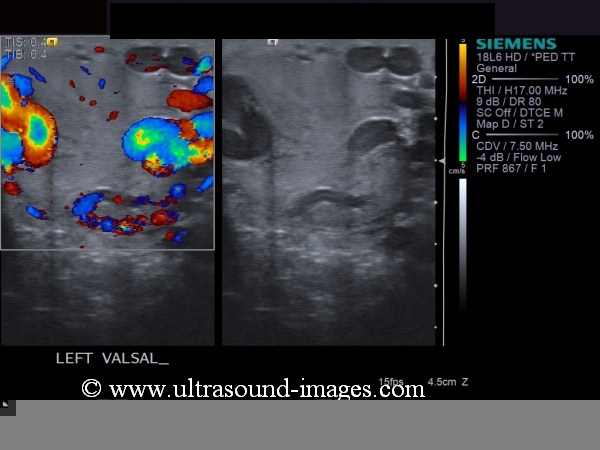
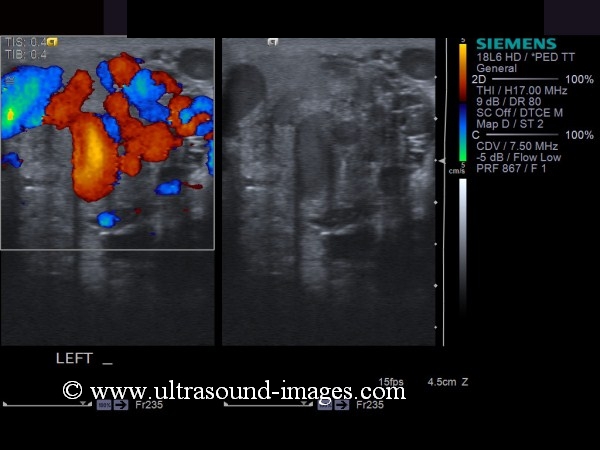
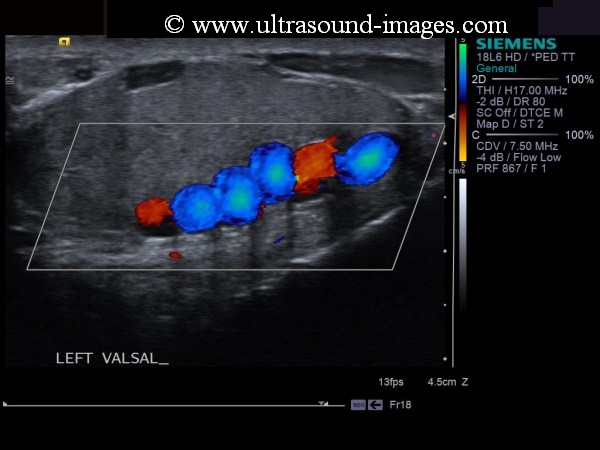
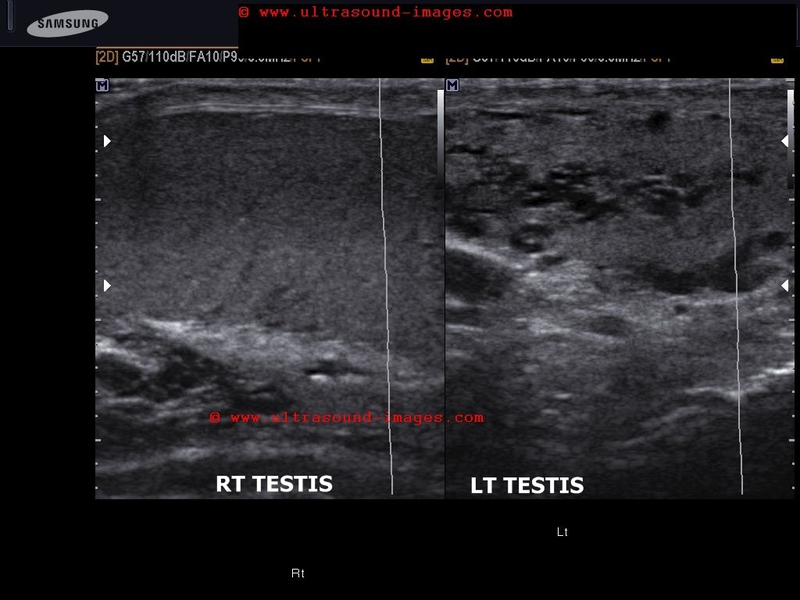
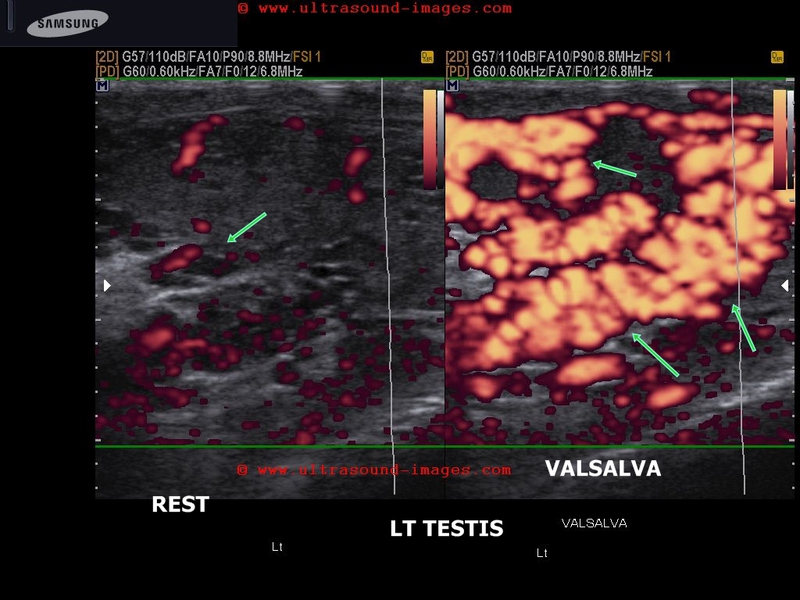
Sonography of the scrotum done on this patient (power Doppler images) of infertility showed: pampiniform plexus veins of diameter 2.2 to 2.4 mm. during the resting state (ie: without Valsalva maneuver) in the left scrotum. On Valsalva maneuver, the veins appear further dilated (measure upto 4.5 mm.). Color Doppler imaging of the scrotum also showed bidirectional flow in the pampiniform veins. Similar changes are seen in the right scrotum (3.3 mm. on Valsalva). The last image (Color Doppler) on lower right shows another patient with bidirectional flow of dilated veins in left scrotum. These ultrasound and Doppler images are diagnostic of bilateral Varicocele (grade 3). The grading (sonographic) we use is: (on Valsalva): Grade-1: 2-2.5 mm. veins Grade-2: 2.5- 3 mm. veins Grade-3: > 3mm. veins
Reference: http://emedicine.medscape.com/article/382288-imaging (a good article).
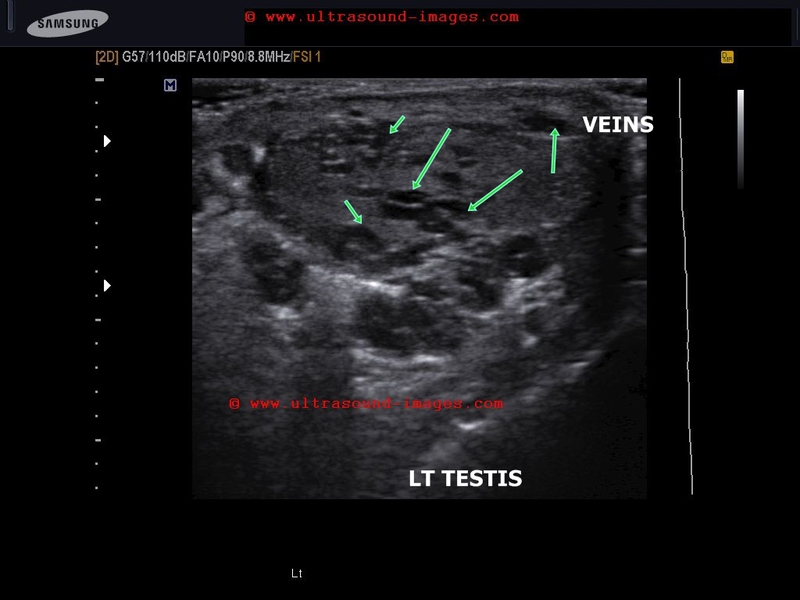
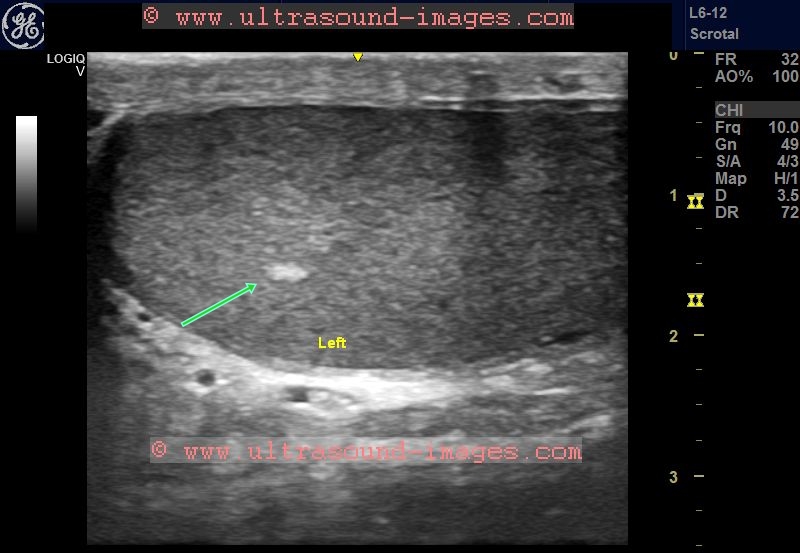
B) Intratesticular varicocele

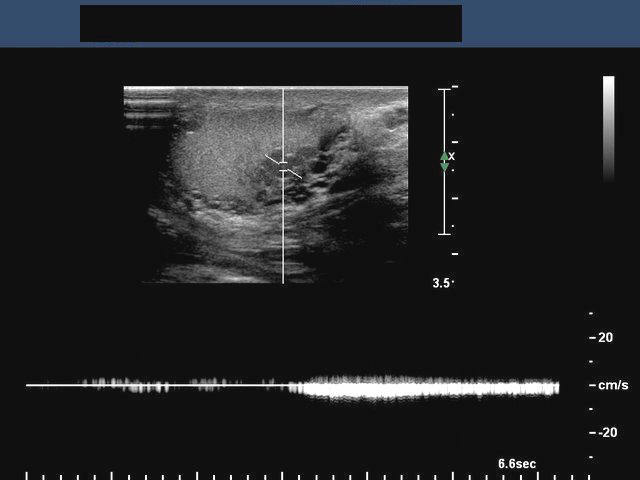
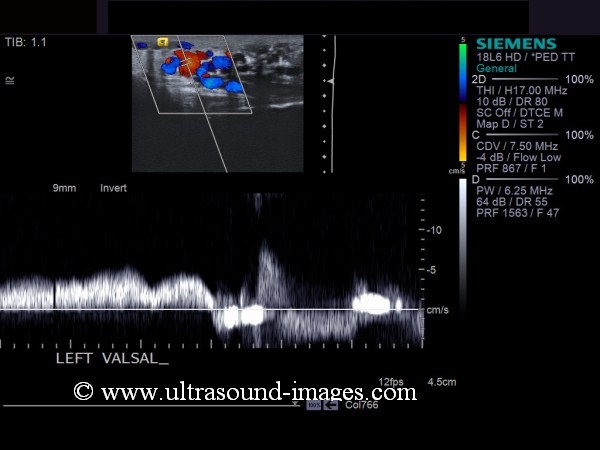
The left scrotum shows a large extratesticular varicocele (long arrow in image on left). Also present are a few dilated vessels (more than 2 mm. each) in the subcapsular part of the left testes (small arrow in color Doppler image). Spectral Doppler trace of the vessels show typical low resistance venous flow pattern. These Color Doppler and spectral Doppler ultrasound images are diagnostic of intratesticular varicocele of left testes. This appears to communicate with the Extratesticular varicocele. Color Doppler helps to rule out other lesions like tubular ectasia of rete testes and Testicular neoplasia which can cause similar appearances on sonography. Both above images are courtesy of Ravi Kadasne, MD, UAE.
Reference:
1)http://drjoea.googlepages.com/scrotum
2)http://www.jultrasoundmed.org/cgi/reprint/24/12/1711 (free article and images)
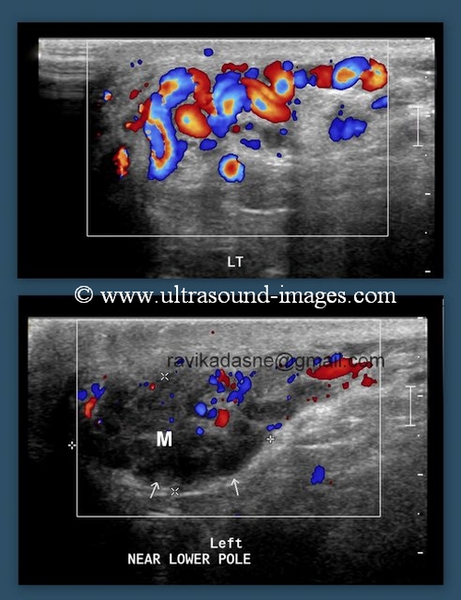
C)intratesticular varicocele- case-2

This is yet another case of intratesticular varicocele (ITV) detected on ultrasound and color Doppler imaging of the scrotum. Intratesticular varicocele is usually left sided and associated with the left testis, which correlates well with the incidence of extratesticular varicocele (ETV) on the left side. Almost all cases of intratesticular varicocele (as in this case too- large arrows) are usually associated with the presence of co-existing extratesticular varicocele (small arrows)- see ultrasound and Doppler flow images above. The large dilated tortuous vessel extending from the mediastinum of the left testis to the periphery, and which shows venous flow pattern on Power or color Doppler is characteristic of intratesticular varicocele. The spectral Doppler flow waveform would also show reversal of flow in the vessel confirming a diagnosis of intratesticular varicocele. Intratesticular varicocele is also often associated with a history of orchidopexy for undescended testis. These images are courtesy of Ravi Kadasne, MD.
The main differential diagnosis in cases of intratesticular varicocele include tubular ectasia of the rete testis, orchitis and simple cyst of the testis. Orchitis would also show flow on color Doppler imaging of the affected testis. However, follow up would help confirm this as flow would return to normal once the inflammation has subsided. Simple cyst of the testis may look similar to a type of intratesticular varicocele which is oval in shape on B mode ultrasound. However, a simple cyst would not show flow on Doppler imaging as is the case with tubular ectasia of the rete testis.
References:
Sonography and Doppler imaging of scrotum- intratesticular varicocele-(journal of ultrasound)
Ultrasound imaging of intratesticular varicocele- AJR
D)thrombosed varicocele
This patient had a painful mass palpable in lower pole of the left testis. Ultrasound and color Doppler imaging of the scrotum revealed grade 3 varicocele with multiple dilatated varicose veins in upper part of left scrotum showing significant flow. However, the lower pole (arrows) shows multiple dilatated pampiniform veins, but these veins do not show flow on Doppler imaging, even with very sensitive PRF settings, suggesting thrombosis. Pampiniform vein thrombosis in a varicocele is a known complication, but is very rare. Images of thrombosis of varicocele are courtesy of Ravi Kadasne, MD.
References:
Imaging in spontaenous thrombosis of varicocele
E)large intratesticular varicocele
Case-5-very severe-left-intratesticular-varicocele

Intratesticular varicoceles are very rare, but a large one such as the case above showing multiple varicose veins in the left testicle, is extremely rare. Spectral Doppler flow also shows considerable flow reversal in the affected intratesticular veins on Valsalva manoeuvre confirming the diagnosis. The ultrasound and Doppler images also show the presence of a grade 3 extratesticular varicocele. These images are courtesy of Shlomo Gobi, Israel.
Case-5 (above) also shows a patient with very severe intratesticular varicocele. The left testis again affected and is literally flooded with the varicose vessels (especially on Valsalva).
Bilobed testes: (Bilobed testicles/ bilobed testis)
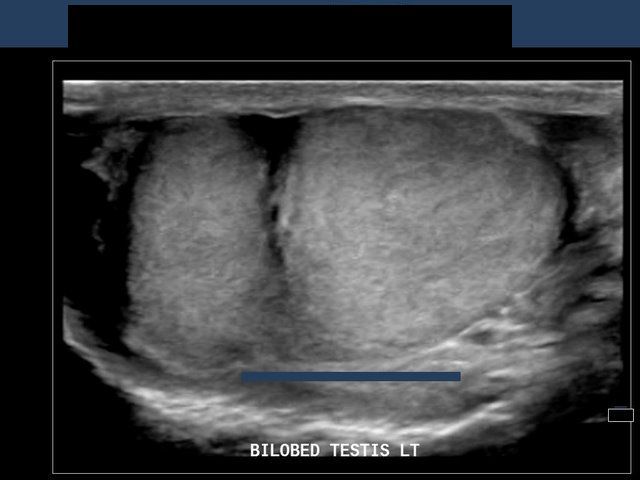

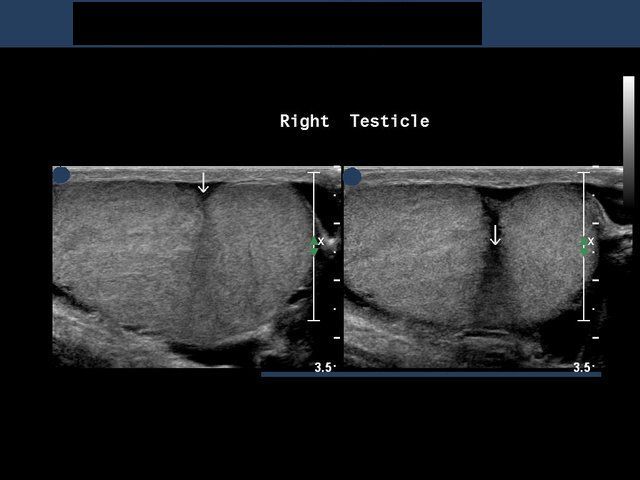
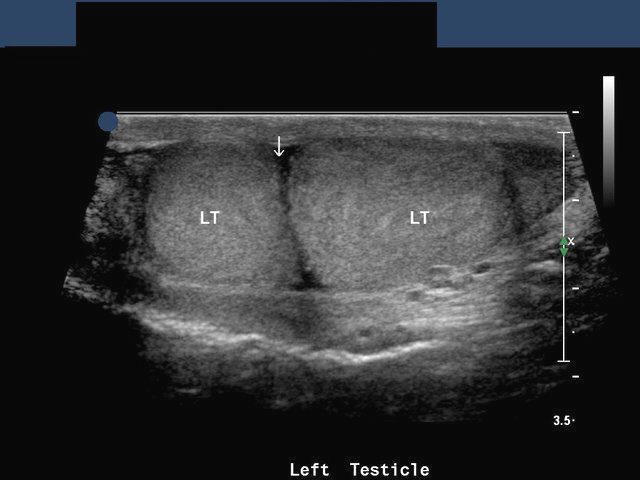
This young male patient underwent sonography of the scrotum (testes). Sonographic images show a deep horizontal cleft (see arrows) passing partially through the testicles on both sides. The tissue on either side of the cleft, bilaterally, show the same echogenicity and echotexture as the normal testes. This appearance is similar to duplication of testes (polyorchism or polyorchidism). The main difference is that in duplication, the supernummerary testes is much smaller in size than the main testicle. Thus these ultrasound images are suggestive of bilateral bilobed testicles (bilobed testes). Ultrasound images taken with a Philips IU 22 ultrasound machine, by Dr. Ravi Kadasne, MD, UAE.
Reference:
http://www.springerlink.com/content/x152371r18845441/
http://resources.metapress.com/pdf-preview.axd?code=x152371r18845441&size=largest
http://drjoea.googlepages.com/gallery-testes(on polyorchidism)
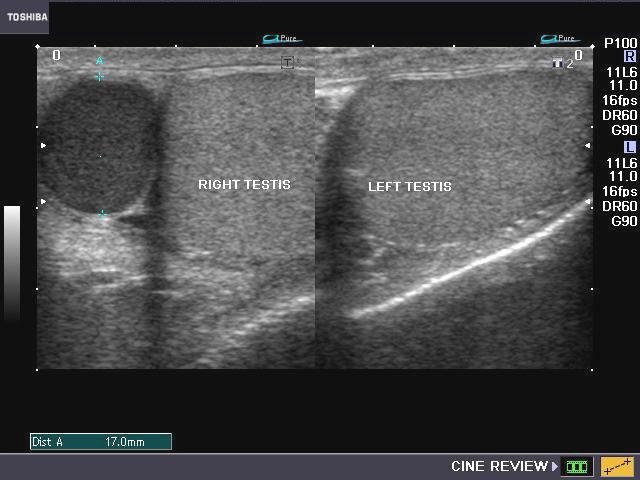
Simple cyst of testes
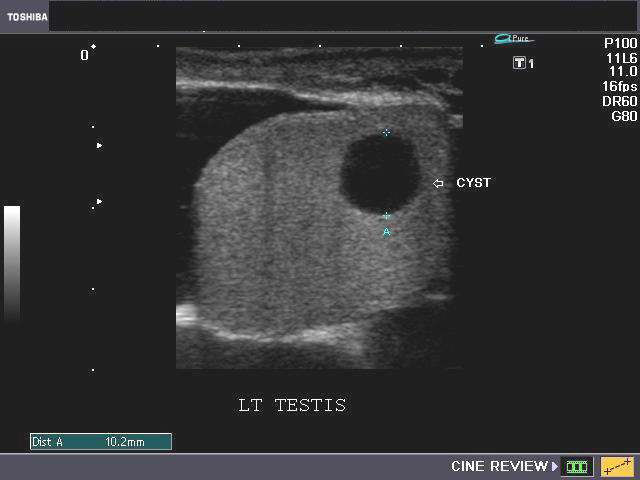
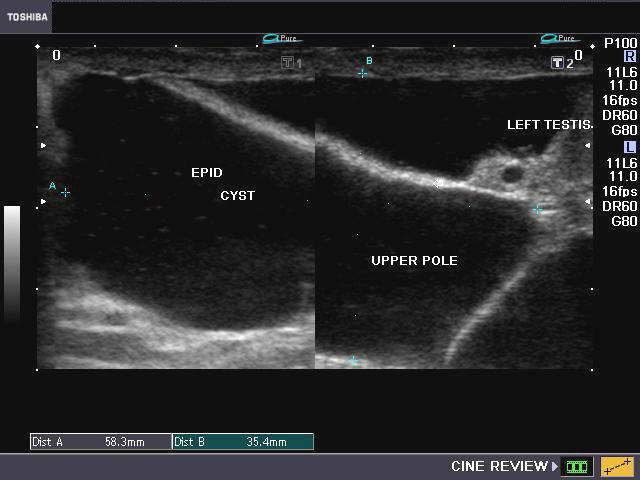
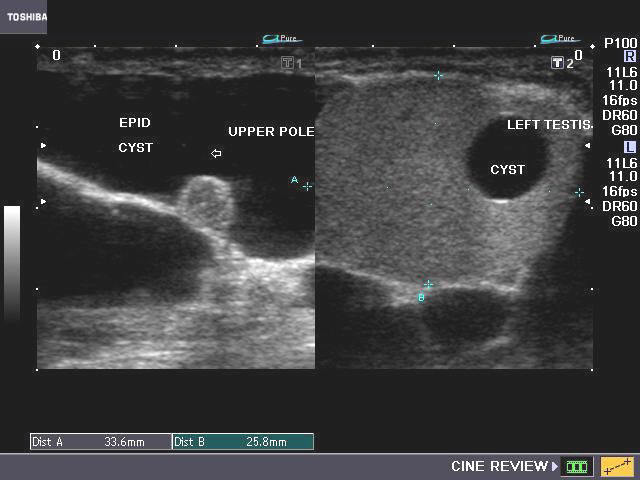
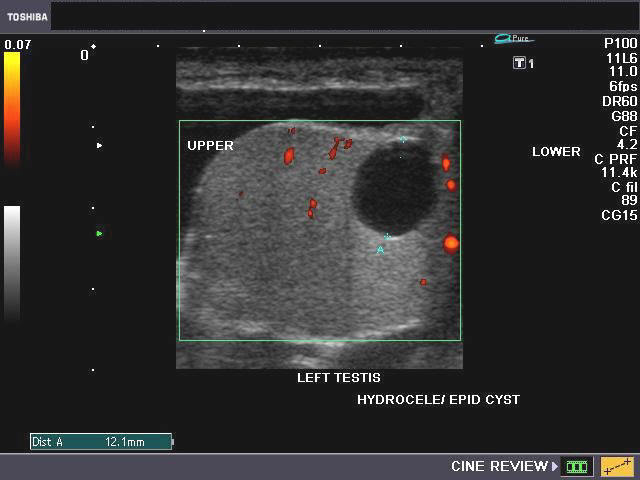
This middle aged male patient had a large swelling of the left scrotum. Sonography showed a huge encysted collection of fluid around the upper pole of left testes with few septae within this. Particulate debris was seen in the fluid collection. These findings suggest large left epididymal cyst or encysted hydrocele of left scrotum. The left testes also shows a solitary cyst of 1 cm. towards the lower pole. The lesion is well within the testicular parenchyma and shows clear fluid content. The margins of the cyst are well defined. These ultrasound findings also suggest a differential diagnosis of simple cyst vs. tunica albuginea cyst of left testes. Simple cysts are usually located close to the mediastinum testes. Power Doppler image shows absence of flow in the anechoic lesion.
Reference:
http://radiographics.rsna.org/content/24/suppl_1/S243.full(free article/ images)
http://www.mypacs.net/cases/TESTICULAR-CYST-3658114.html(free article/ image)
Cryptorchidism
Cryptorchism is the failure of the testis, on one or both sides, to descend from the abdomen to its proper position within the scrotum. This is broadly classified into 2 types:
A) Ectopic testis: here the testis may be located in an abnormal position- femoral, transverse scrotal, perineal and prepenile.
B) True undescended testis is either: abdominal, inguinal (within the inguinal canal), or suprascrotal ( just above the scrotum).
inguinal testis
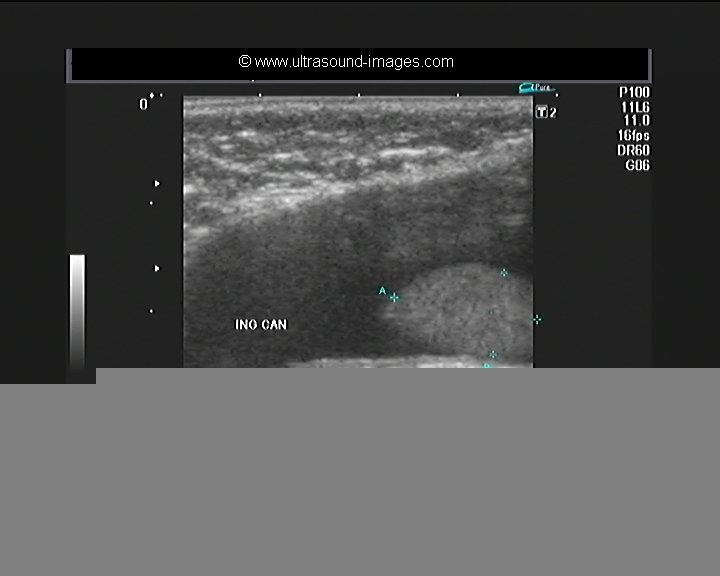
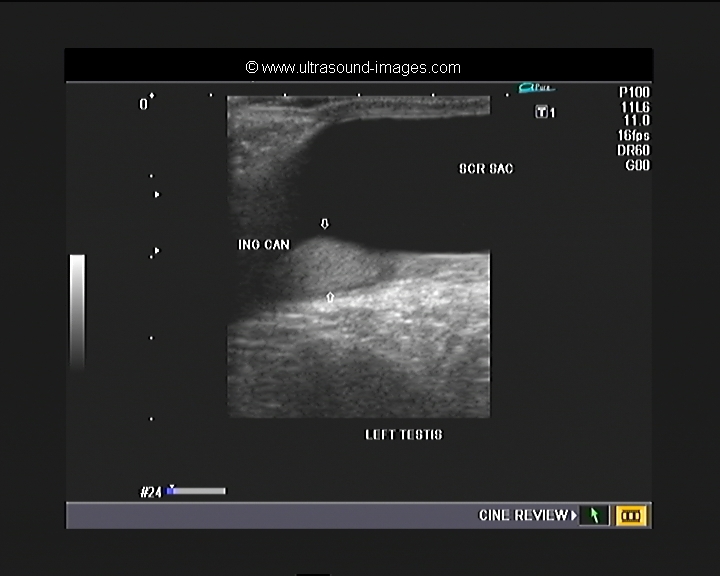

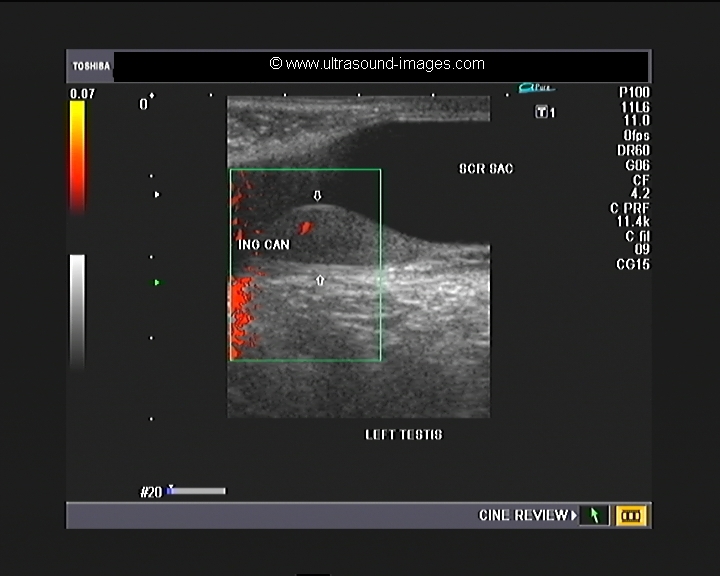
this is an example of the left inguinal testis (see ultrasound images of left inguinal testis below). in this infant, aged two months, the baby has normal rights testis located within the scrotal sac. However, the left testis is located low down within the left inguinal Canal suggesting left cryptorchidism or left undescended testes. Also evident is communicating hydrocele of the left side. Normal vascularity is present in the left testes suggesting that this testis is viable.
cryptorchidism-case-2
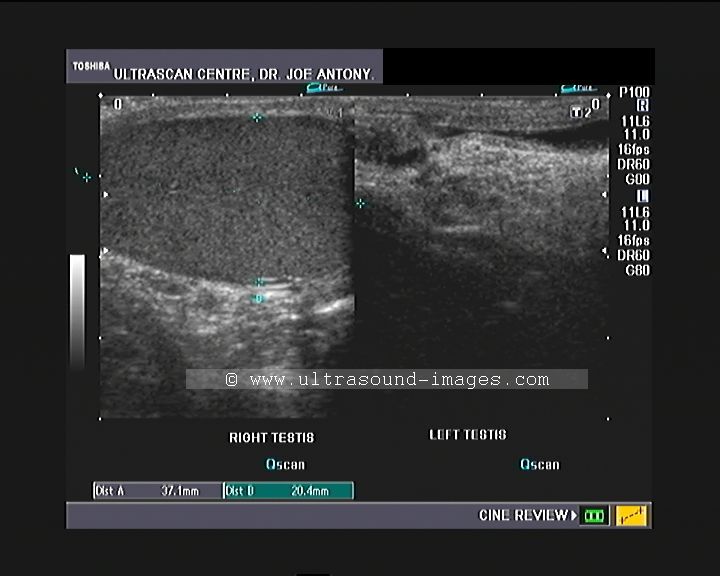
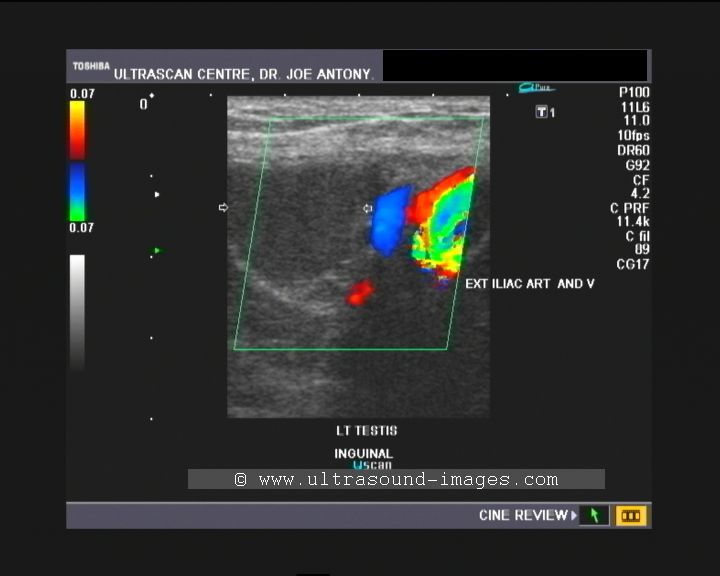
This 21 year old male patient shows absence of the left testicle in the left scrotum (see ultrasound image above). Search for the missing left testicle revealed the left testis to be present in the lateral part of the left inguinal canal. This undescended left testicle (a type of cryptorchidism) is seen to be adjacent to the left external iliac vein and artery (see color Doppler ultrasound image above). In this case of cryptorchidism the left inguinal undescended testicle is smaller in size as compared to the right testicle.
Ultrasound images of abdominal testis
Case-1
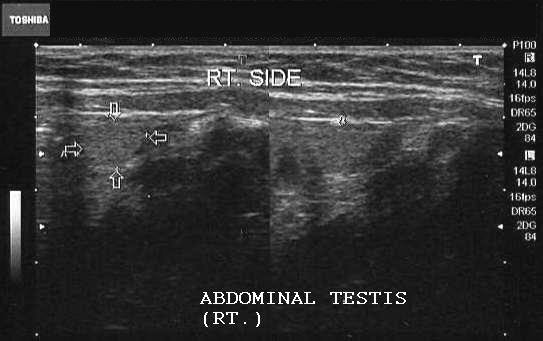
Sonography of the scrotum showed the left testis in its normal position within the scrotum. The right testis was not visualized within the scrotum but located just above the right inguinal canal (abdominal testis) (arrows).
Case-2
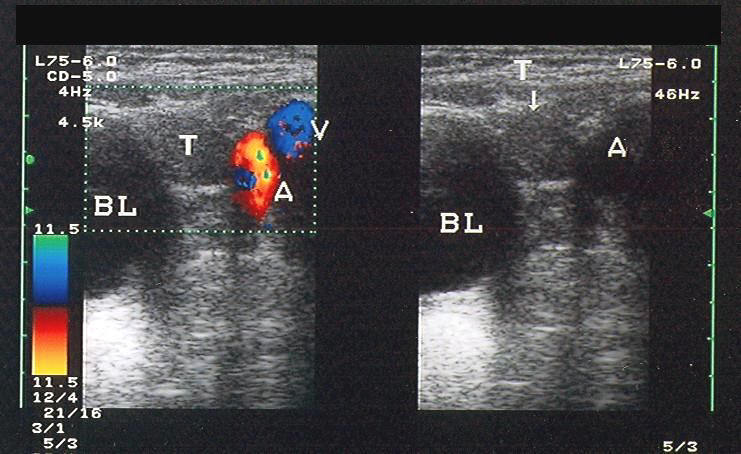
The left testis (T) is seen within the abdomen in close proximity to the urinary bladder (BL) s/o abdominal testis. The testis is seen as a hypoechoic structure with mediastinal echoes. The two main complications/ sequelae of undescended testes are: infertility and increased risk of malignancy. (A= Left external iliac artery; V= Left external iliac vein)
Snapshot of case-2: The left abdominal testis is visualized
All above images are courtesy of Dr. Ravi Kadasne, UAE.
Reference:
1)http://emedicine.medscape.com/article/377971-imaging
2)http://emedicine.medscape.com/article/377971-overview
Retractile testis


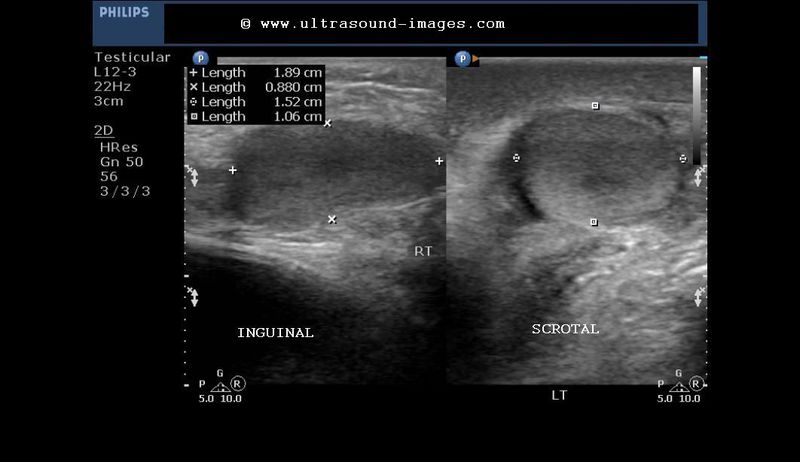
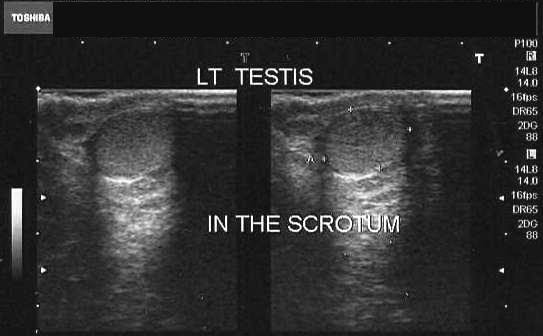
This 6 year old child had left scrotal pain. Ultrasound images of the scrotum show a small left epididymal cyst with mild epididymitis. The right testis was not visualized in the scrotum. A sonography of the groin showed the missing right testis in the right inguinal canal. However, a short time later, the right testis was visualized in the right scrotum. However, it again returned to its position in the inguinal canal. These ultrasound images show the empty right scrotum with the right testis in the inguinal canal. The retractile testis is not an ectopic testis as the movement of the right testis (in this case) between the scrotal position and its inguinal position are transient. Usually the retractile right testis will permanently return to its scrotal position. The movement of the retractile testis is due to transient contraction of the cremaster muscle. In such cases, manually guiding the retractile testis to its scrotal position, is a painless affair, unlike true inguinal (undescended) testis.
Reference:http://www.mayoclinic.com/health/retractile-testicle/DS00742
Tubular ectasia of rete testes
(Also known as: cystic transformation of rete testis)
Tubular dilatation of the tubuli recti of the testes
Case- 1



Reference:
http://radiographics.rsna.org/content/21/suppl_1/S273.full.pdf+html (free article and images)
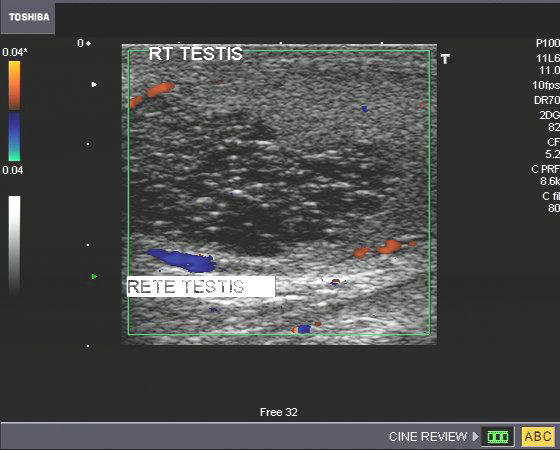
Case-3: Cystic transformation of rete testis (right testis)


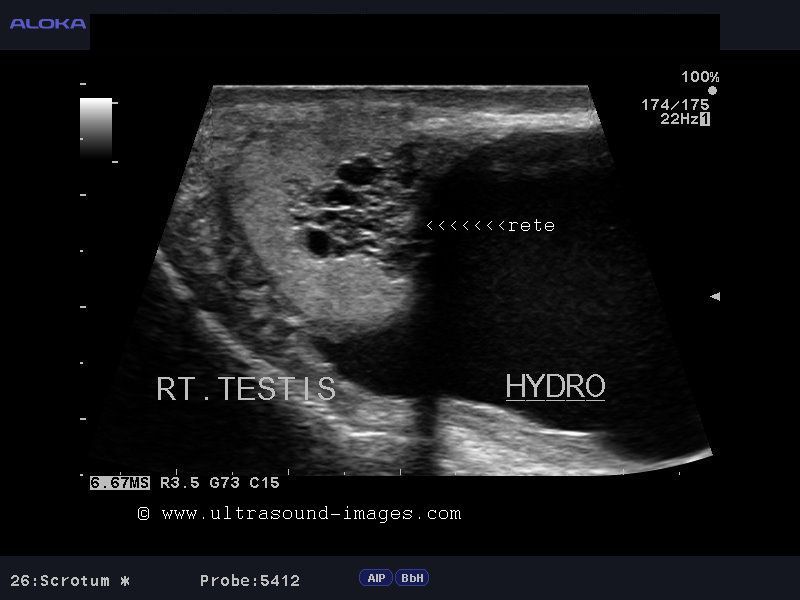
These ultrasound images show a similar case of cystic transormation of rete testis (right sided); this is synonymous with the term - tubular ectasia of rete testis. In addition to the tubular ectasia there is a large cystic area in the right scrotal sac. This could represent a hydrocele or a large spermatocele. The presence of echogenic particles in this fluid might favor spermatocele. One of the causes of tubular ectasia of rete testis includes history of vasectomy. Usually cystic transformation of the tubules of the rete testes is bilateral; however it may be unilateral as in this case. Note the typical elongated cystic areas in the mediastinum of the right testis. A close differential diagnosis in such cases can be cystic teratomas of the testis and malignant cystic testicular neoplasia. The ultrasound images in this case study are courtesy of Dr. Jaydeep Gandhi, MD, India. (The ultrasound equipment used here is the Aloka Prosound Alpha 7 system).
References:
http://www.sonographers.ca/COW.php?post=24
Tubular ectasia of the testicle- Ultrasound and MR imaging- AJR
Atrophy of testis


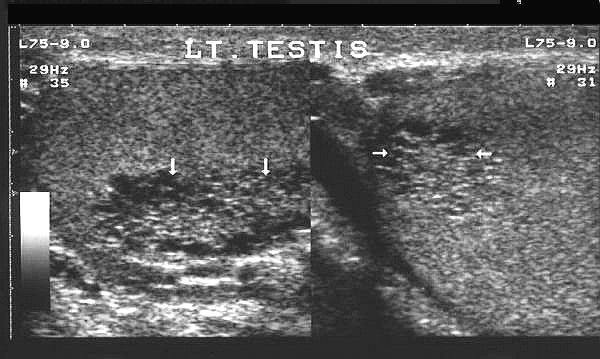
This middle aged man had a previous history of mumps orchitis of the right testis. Following this the affected organ became small in size. When he presented to us, he had a history of infertility and low sperm count. Ultrasound and color/ Power Doppler images show a normal left testis; the right testis is small in size (compared to its fellow). The right testis is also hypoechoic and shows poor vascularity. These ultrasound findings suggest a diagnosis of post mumps atrophy of the right testis. This patient also had a bilateral grade- 2 varicocele. Atrophy of the testes is a known complication of mumps related orchitis. Testicular atrophy following mumps is usually patchy and often does not cause infertility.
Reference: http://www.springerlink.com/content/gpmxfe2wgb5ep0fj/ (free abstract)
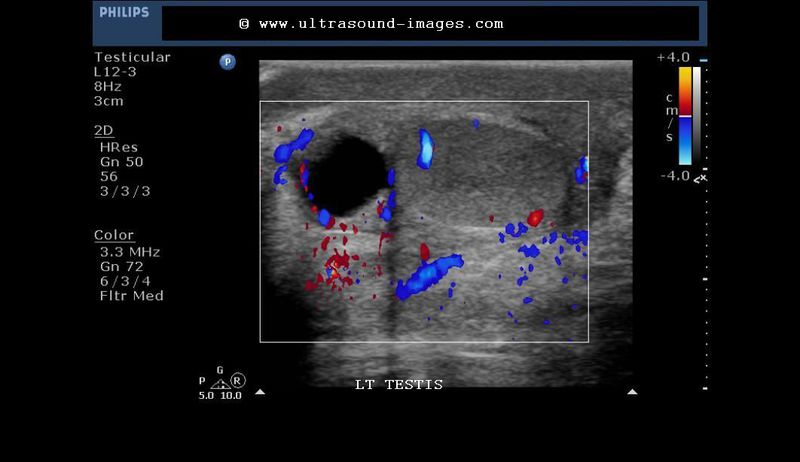
AVM of testis (intratesticular arteriovenous malformation)
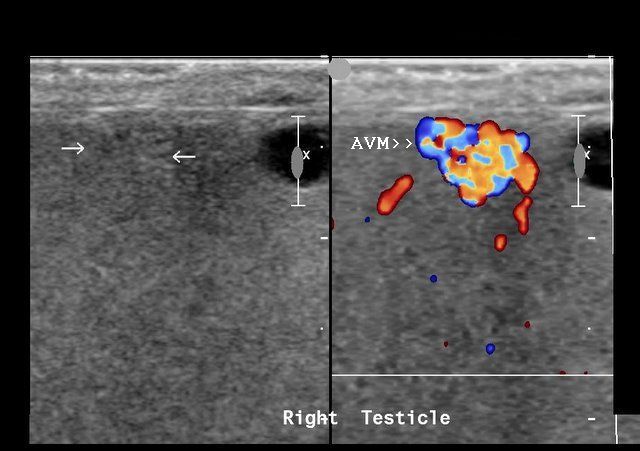
Ultrasound of the right testicle in this patient shows hypoechoic area in the anterior part of the organ (left half of the ultrasound image). The right half of the image (Color Doppler) shows a small mass of vessels in this lesion with a draining vein. This appearance can be caused by only 3 lesions of the testis. One of them is an intratesticular varicocele. This is usually associated with an extratesticular varicocele (not seen in this case). The other possibilities are that of a hemangioma or arteriovenous malformation. Both are very rare lesions of the testis. The presence of a draining vein suggests arteriovenous malformation as a diagnosis in this patient. Besides, there is no significant testicular enlargement in this case ( a sign found in hemangioma of the testes). Ultrasound and Color Doppler images are courtesy of Dr. Ravi Kadasne, MD, UAE.
Reference: http://www.jultrasoundmed.org/cgi/reprint/22/3/295.pdf(free article and images).
Orchiopexy (orchidopexy)
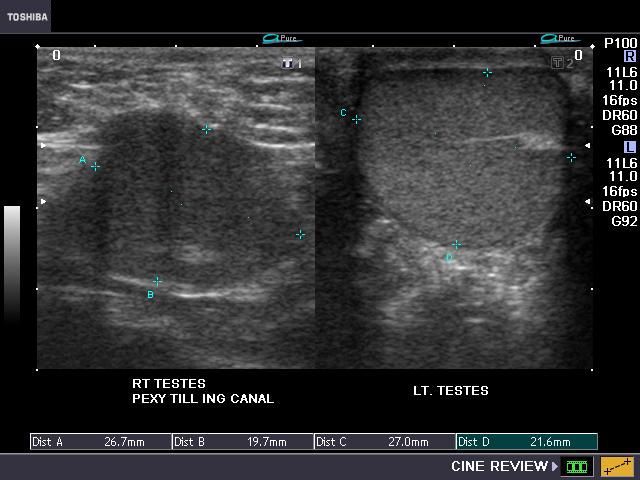

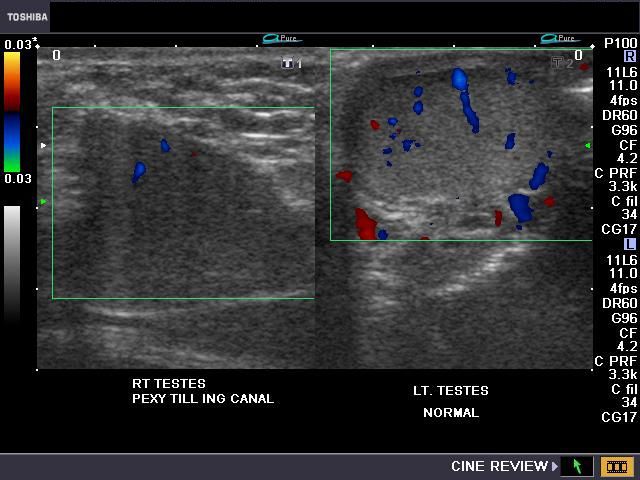
This young adult male patient had a high abdominal right testis for which he underwent orchiopexy. The ectopic right abdominal testis was relocated to the right inguinal canal due to lack of sufficient length of the testicular vessels. Ultrasound and color Doppler images of the testes show normal left testis. However, the right testis shows poor vascularity and is hypoechoic. These ultrasound appearances suggest possible atrophic changes in the right testis.
References:
http://emedicine.medscape.com/article/438378-treatment(free article)(free article)
http://www.aafp.org/afp/20001101/2037.html
Indirect inguinal hernia forming large Right scrotal swelling



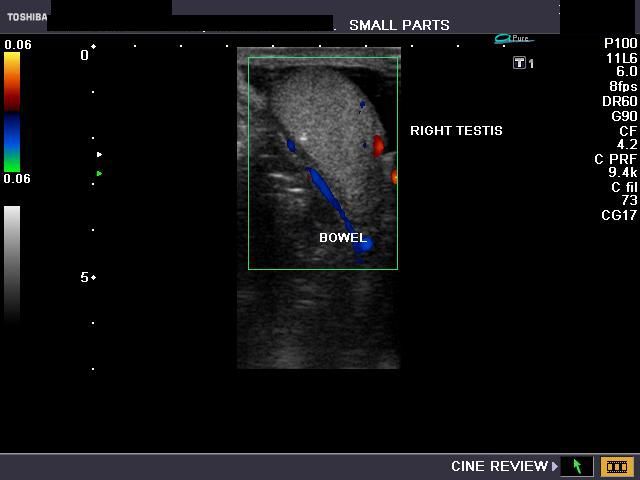


This patient presented with a large right scrotal swelling of a year's duration. The mass was non tender. Ultrasound images (above) show echogenic tubular structures with peristaltic movement within the right scrotum. This appearance was typical of small bowel. Color Doppler shows normal vascularity of the right testis which is pushed downwards. This ultrasound appearance/ images are typical of a large right indirect inguinal hernia. In this case the hernial sac has pushed through the inguinal canal on the right and descended into the right scrotum. There is also evidence of bilateral small hydroceles.
You can view the ultrasound video clip of this case of indirect inguinal hernia above:
References:
http://radiographics.rsna.org/content/21/suppl_1/S261.full.pdf+html (free article)
http://www.ajronline.org/cgi/reprint/187/1/185(free article on hernia)
Epidermoid cyst of testis

This patient presented with a painless swelling of the right testis. Ultrasound image shows a rounded complex mass with a characteristic "onion peel" appearance due to layers of hypoechoic and hyperechoic tissue elements alternating with each other. This ultrasound image with the typical onion peel appearance of the mass is diagnostic of epidermoid cyst of the testis. Some epidermoid cysts do not have this typical onion peel appearance but rather a heterogenous echotexture. Other cases of epidermoid inclusion cysts may have a hypoechoic appearance with echogenic ring of calcification. Epidermoid inclusion cysts or epidermoid cysts are benign and can occur at any age group, though they are more common in the age group 20 to 40 years. Epidermoid cysts of the testis are extremely rare with an incidence of 1 % of all testicular masses. They are a variant of teratodermoid tumors with a primary epidermal tissue element. Though keratin is usually present in epidermoid cysts of the testes, these lesions do not contain hair or sebaceous cysts. Ultrasound image of epidermoid inclusion cyst is courtesy of Dr. Ravi Kadasne, MD, UAE.
References: Sonoworld article on sonography of epidermoid cysts of testes
hydrocele with display of spermatic cord

This ultrasound image shows a large hydrocele with the spermatic cord imaged coursing through the fluid. Image is courtesy of Ravi Kadasne, MD.
filarial-dance-scrotal
Ultrasound imaging video showing filarial dance produced by live filarial parasites in the scrotum near epididymis. The sonographic video below shows linear, twirled, echogenic structres (the live filarial worms) within a dilated and partially obstructed lymphatic channel (seen as the cystic fluid filled structure in the scrotum). The active movement of the linear echogenic structures is called the filarial dance sign. On treatment with diethylcarbamazine, the drug of choice for the treatment of filariasis, this lesion disappeared suggesting a resolution of the filarial infestation. This ultrasound video of filarial dance is courtesy of Gunjan Puri, M.D.
References: Sonographic imaging of filarial dance
macro-calcification-testis



Middle aged man shows macro-calcification (or large calcific lesion) of the left testis in above ultrasound images.
Microliths of the testis are known to be linked to higher incidence of testicular malignancies.
Recent studies suggest even macro-calcification of the testis is associated with significant higher incidence of testicular cancers.
Macro-calcific lesions of the testis are a very rare occurence compared to microliths.
Macro-calcifications of testis are those measuring > 3 mm in size.
References: Testicular macro-calcifications sonography
© 2026, Joe Antony, MD All images and content in this site are copyrighted. www.ultrasound-images.com When visiting this site, we may use cookies to improve the performance of this site. Use of this site means you accept the use of cookies. Read our privacy policy at this page: https://www.ultrasound-images.com/privacy-policy/