
Thyroid
Contents of this page
- Agenesis of the thyroid
- Hemiagenesis of the thyroid
- Dysgenesis of thyroid- ectopic thyroid tissue
- Hashimoto's thyroiditis
- Hashimoto's thyroiditis- Lymphocytic infiltration
- Case-2: Lymphocytic infiltration in Hashimoto's thyroiditis
- Hyperthyroidism-Graves-disease
- Multinodular goiter
- Ultrasound and color doppler imaging of multinodular goiter
- Sublingual thyroid
- Ultrasound image of hemithyroidectomy
- Superficial neck masses- lipoma
- Hemorrhagic colloid cyst of the thyroid
- Malignant thyroid nodule
- Benign nodules of the thyroid
- Case-3: Adenomatous or colloid nodule of left lobe- 3D ultrasound and elastogram
- Toxic thyroid nodule
- Ectopic thyroid tissue
- Parathyroid adenoma
- Case-2 : Parathyroid adenoma in child
- Thyroglossal duct cyst
- Thyroglossal duct cyst inflammation/ abscess
- Branchial cleft cyst or Branchial cyst
- Sonographic atlas of the thyroid
Agenesis of the thyroid


Sonography of the thyroid in this 1 yr. old female child revealed congenital absence of the entire thyroid. Note the empty fossae where the right and left lobes would normally lie. The carotid artery and jugular vein of both sides are seen in the color doppler images. These ultrasound and color doppler images suggest congenital agenesis of the thyroid.
Reference: http://content.nejm.org/cgi/content/abstract/321/1/13(free abstract).
Hemiagenesis of the thyroid
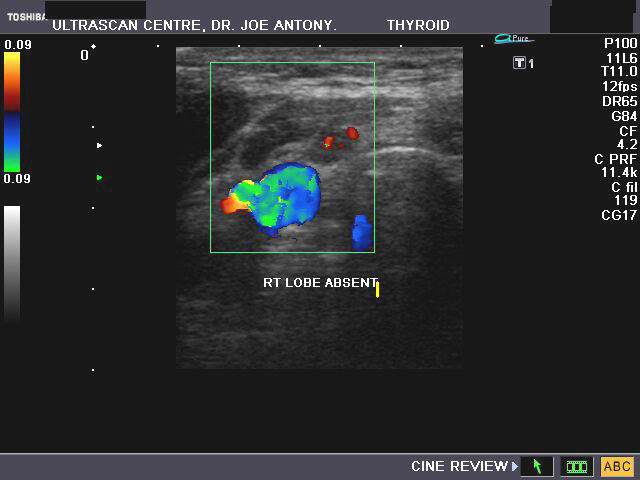


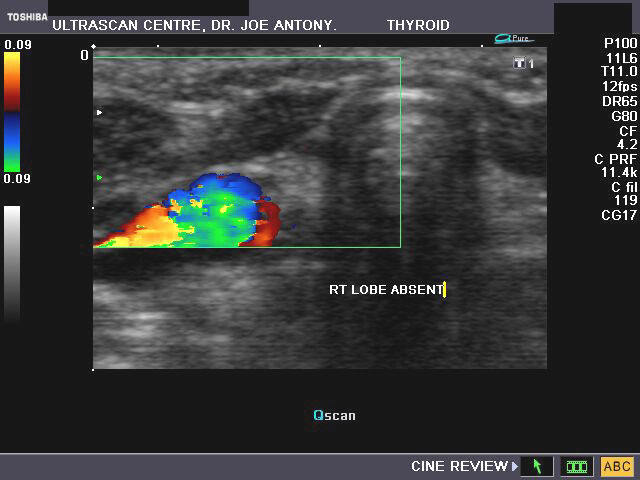
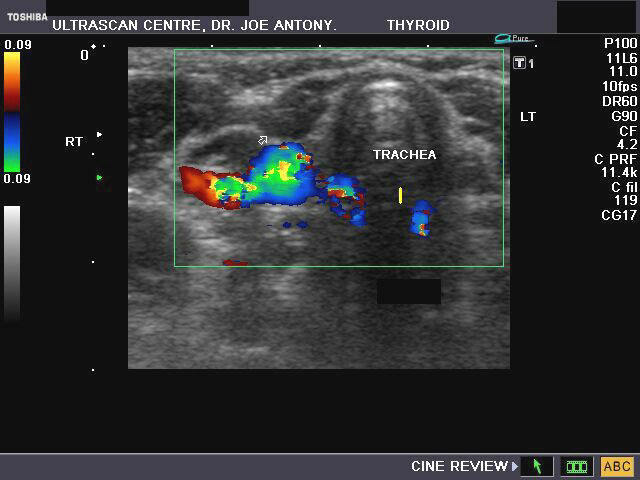
This 18 yr. old female patient presented with symptoms of hypothyroidism. On sonography of the thyroid, we observed: 1) absence of the right lobe of thyroid 2) normal or slightly enlarged left lobe and isthmus of thyroid c) mild to moderate augmentation of vascularity of the left lobe on color doppler imaging. These ultrasound images favor a diagnosis of congenital absence of the right lobe or hemiagenesis of the right lobe with Hashimoto's thyroiditis. This condition is found typically in females with left lobe usually absent.
Reference: 1) http://medind.nic.in/iaw/t05/i2/iawt05i2p53.pdf (free article and images)
Dysgenesis of thyroid- ectopic thyroid tissue


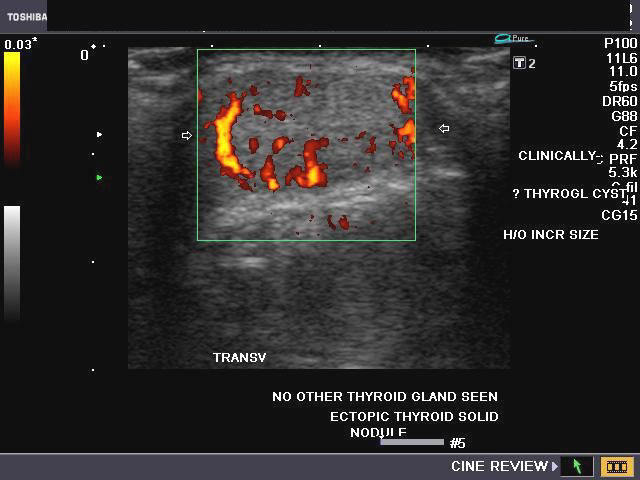
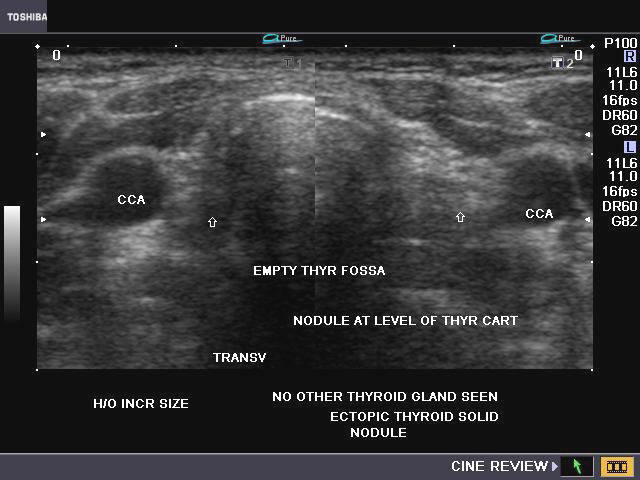

This young, adult female patient complained of a midline swelling of the neck. Clinically, the nodule was palpated in the midline, at the level of the thyroid cartilage and moved with swallowing (deglutition). Ultrasound images of the nodule showed it to be solid, with no cystic areas or calcification. Power Doppler imaging showed moderate vascularity of the nodule. The echogenicity and echotexture of the lesion was same as that of normal thyroid tissue. The thyroid fossa was empty with none of the normally located (orthotopic) thyroid seen. The nodule was long along the sagittal axis (4 x 2 x 1 cms.). These ultrasound images suggest dysgenesis of the thyroid with ectopic thyroid tissue in the midline of the neck. This tissue appears to show goitrous enlargement and appears to be the only available thyroid tissue in this patient.
Reference: http://www.medcyclopaedia.com/library/topics/volume_vi_2/e/ectopic_thyroid.aspx
Hashimoto's thyroiditis

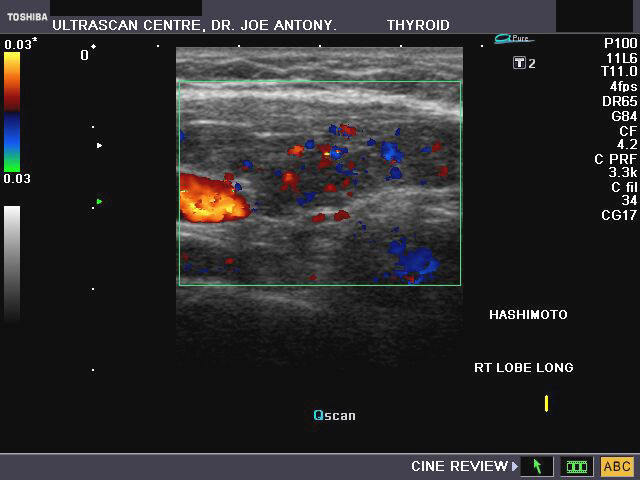
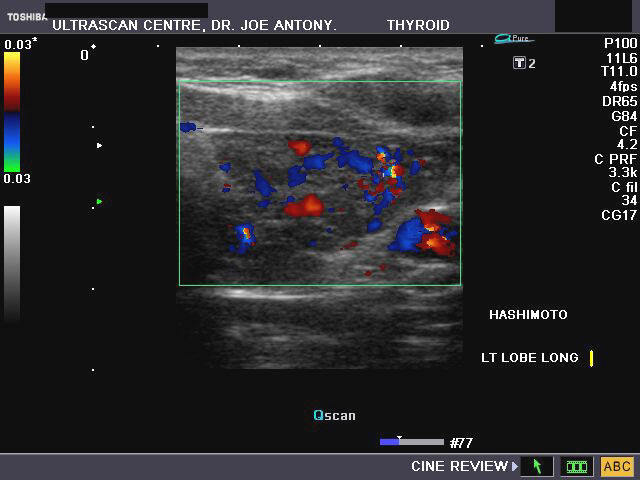
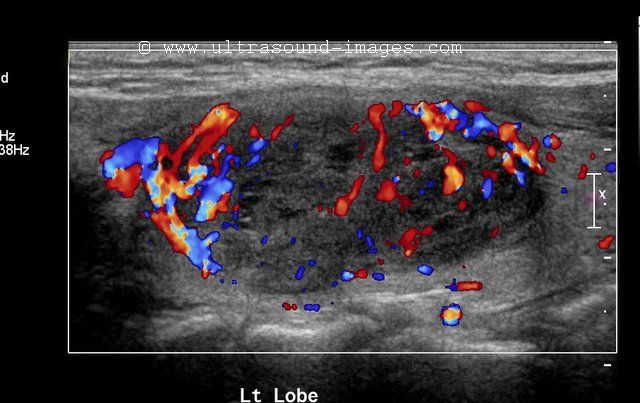
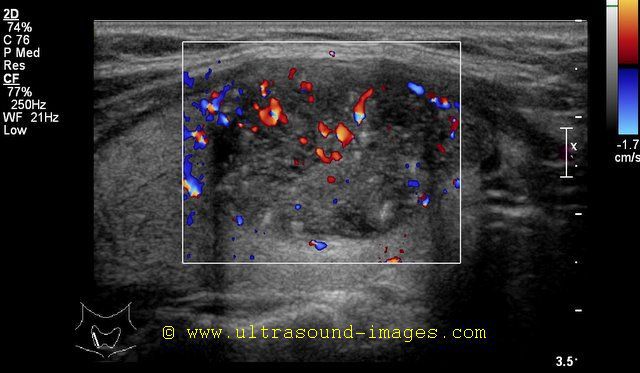
Sonography of the thyroid gland in this middle aged female patient reveal: 1) hypoechoic thyroid gland 2) coarse echotexture of the gland 3) fine linear echoes within the thyroid parenchyma s/o fibrosis 4) Color doppler imaging reveals augmentation of the vascularity of the thyroid gland. These ultrasound images are diagnostic of Hashimoto's thyroiditis. Images taken using a Toshiba Nemio- XG color doppler machine. Hashimoto's thyroiditis is often a cause of decreased thyroid function or hypothyroidism and is thus a causative factor in the development of obesity. Both type1 and type 2 diabetes may be associated with Hashimoto's thyroiditis.
Reference:
1) Hashimoto's thyroiditis article (free article and images)
2) http://www.emedicine.com/med/TOPIC949.HTM(free article and images)
3) http://journal.diabetes.org/clinicaldiabetes/v18n12000/pg38.htm
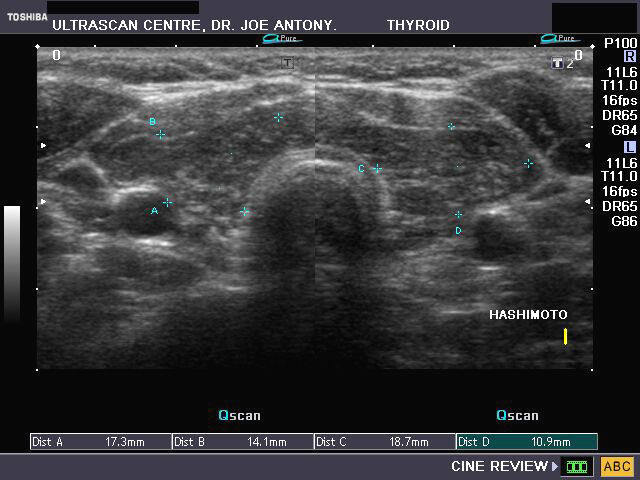
Hashimoto's thyroiditis- Lymphocytic infiltration
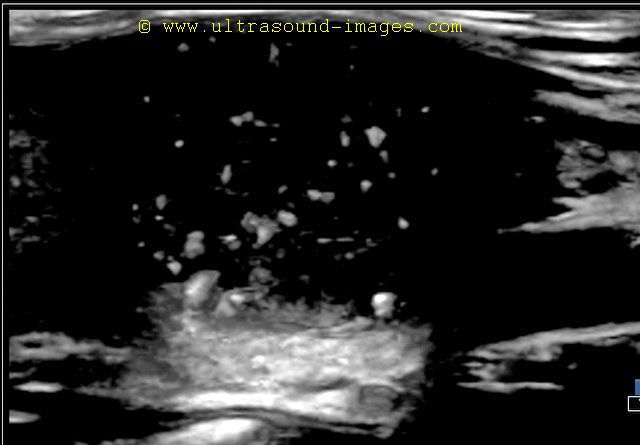
This thyroid shows typical diffuse patchy hypoechoic lesions throughout the gland. This sonographic appearance is called a leopard skin pattern and is seen in lymphocytic infiltration of the thyroid in Hashimoto's thyroiditis. The hypoechoic lesions within the thyroid are areas of lymphocytic infiltration of the thyroid tissue. Ultrasound images of lymphocytic infiltration of the thyroid are courtesy of Dr. Mohamed Sheriff.
References: Ultrasound imaging in Hashimoto's thyroiditis (radiographics article).. article and images
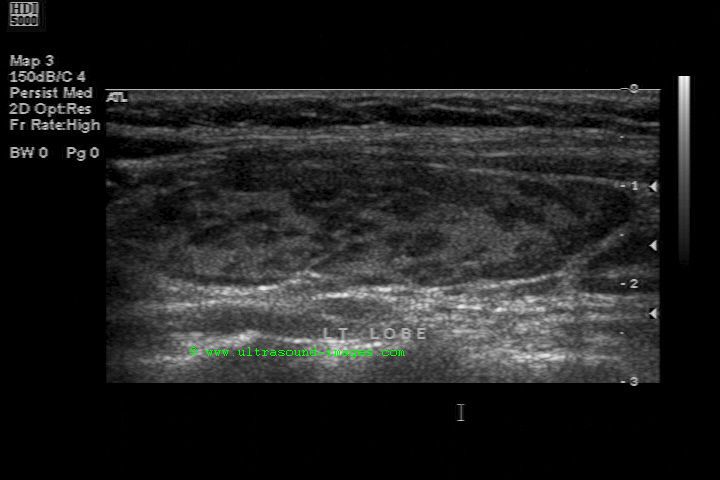
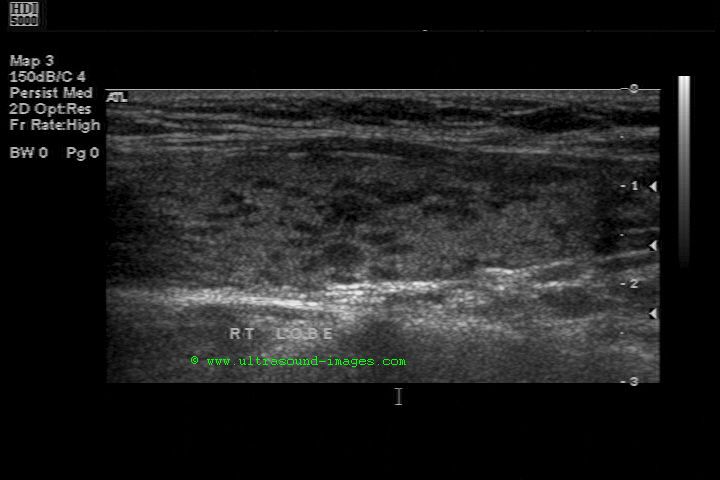
Case-2: Lymphocytic infiltration in Hashimoto's thyroiditis
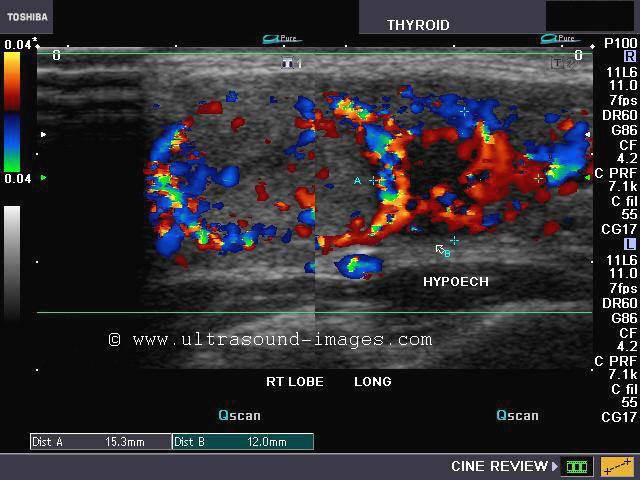
B-mode high resolution images of the thyroid: patchy hypoechoic lesions- the leopard skin pattern


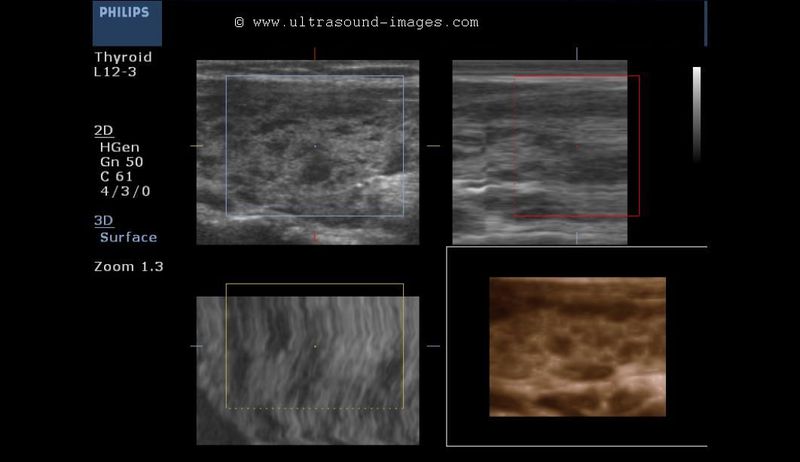
3D- ultrasound images of the thyroid showing patches of lymphocytic infiltration (orange color in lower right quadrant)

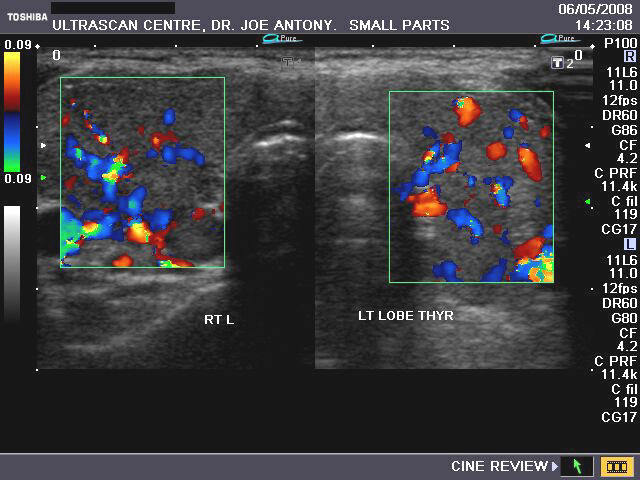

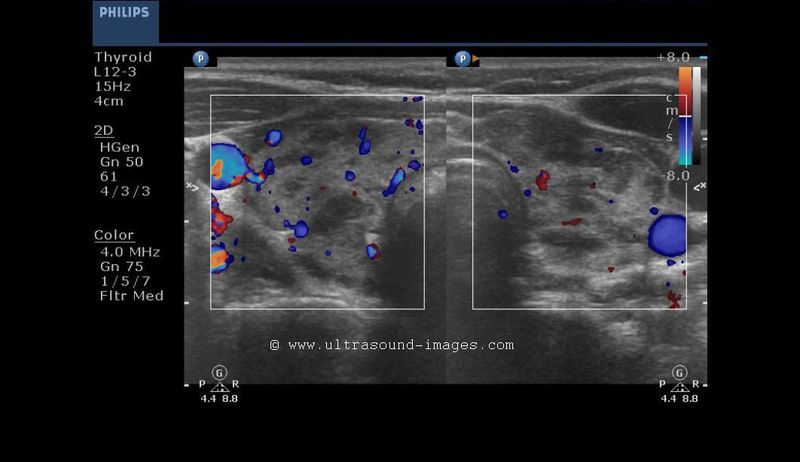
These ultrasound/ color doppler images (taken with a Nemio-XG color doppler scanner), reveal markedly increased vascualrity throughout the thyroid gland. Some degree of inhomogeneity is also present. The patient was a middle aged female with typical features of thyrotoxicosis. Ultrasound images are diagnostic of hyperthyroidism.
Reference:http://www.emedicine.com/Radio/topic315.htm (free article)
thyrotoxicosis-case-2

Another example of a young woman with hyperthyroidism. Observe the diffusely enlarged, inhomogenous thyroid with marked vascularity on color Doppler ultrasound- the so called thyroid inferno.
Graves-disease-thyrotoxicosis-case-3
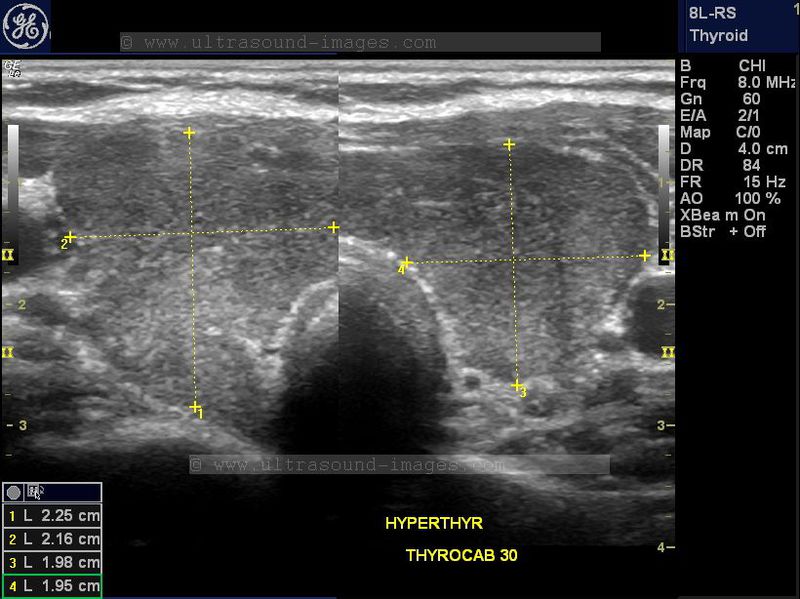
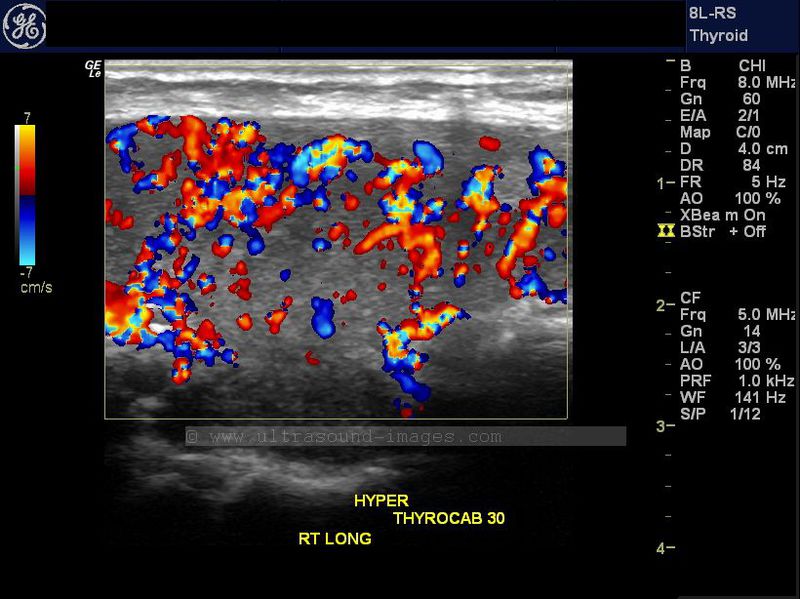

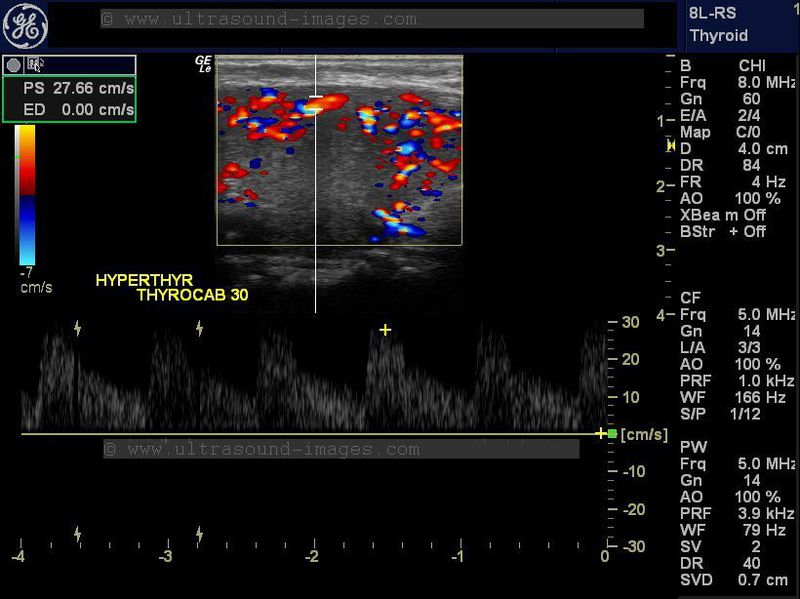
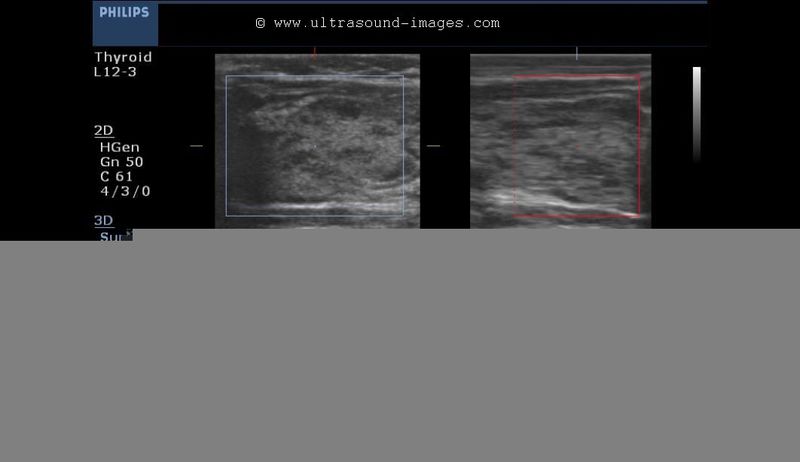
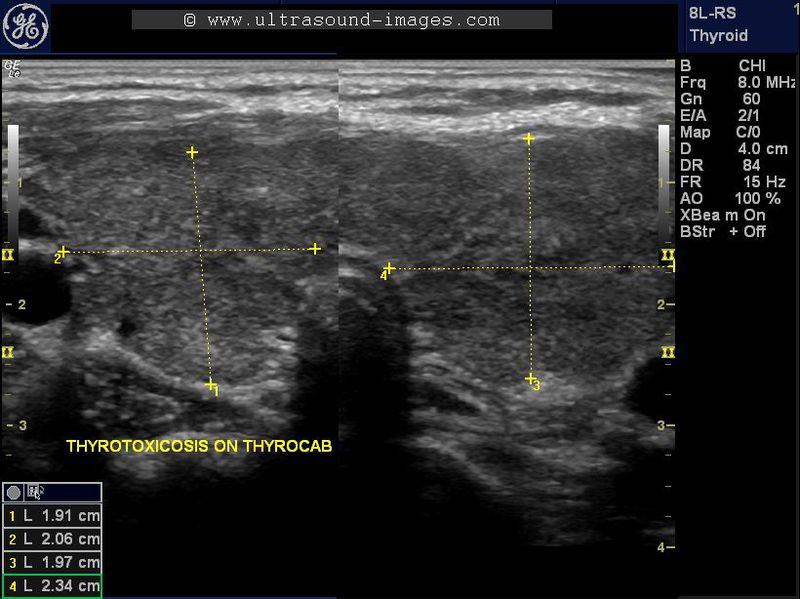
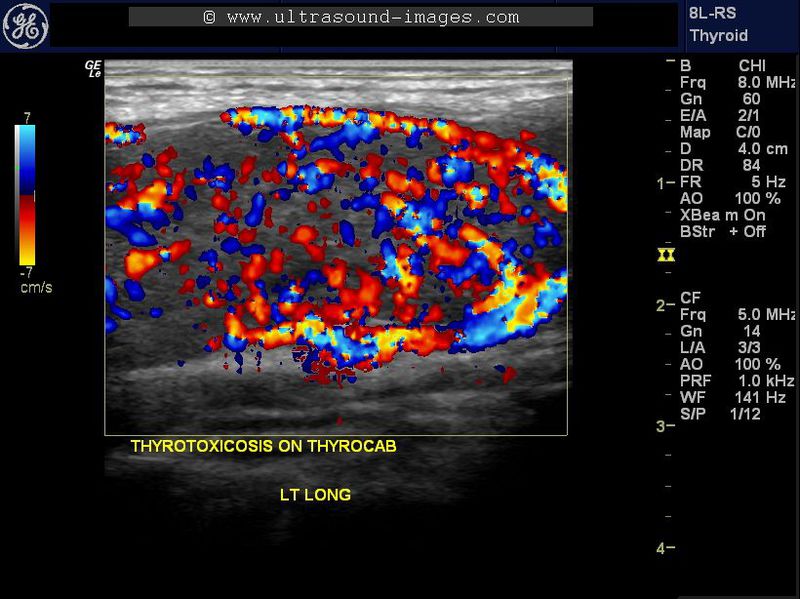
This is yet another case of Grave's disease or thyrotoxic goiter on medical treatment with thyrocab. Despite undergoing therapy for thyrotoxicosis, the thyroid shows markedly increased vascularity on color Doppler and is mildly and diffusely enlarged. The patient is a young woman showing some of the clinical features of Grave's disease. An important differential diagnosis in this case is Hashimoto's thyroiditis which in certain cases may show marked vascularity. However, in this case, the PSV of the thyroid arteries is greater than 30 cm/sec. favoring a diagnosis of Grave's disease.
Multinodular goiter

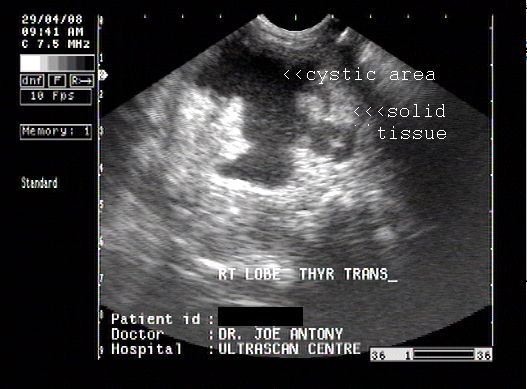
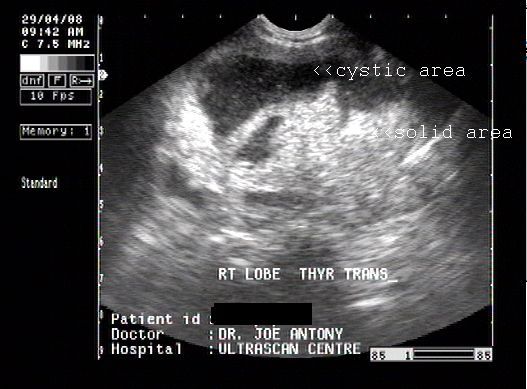
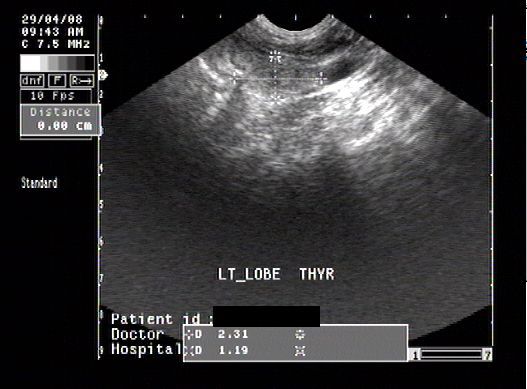
The above ultrasound images show- 1) a huge complex mass (8 x 6 cms.) containing both cystic and solid areas, in the right lobe of the enlarged thyroid. 2) relatively spared left lobe which shows normal size, but has fine nodularity. These ultrasound images are highly suggestive of a multinodular goitre.
http://www.patient.co.uk/showdoc/27000670/ (free article)
Ultrasound and color doppler imaging of multinodular goiter

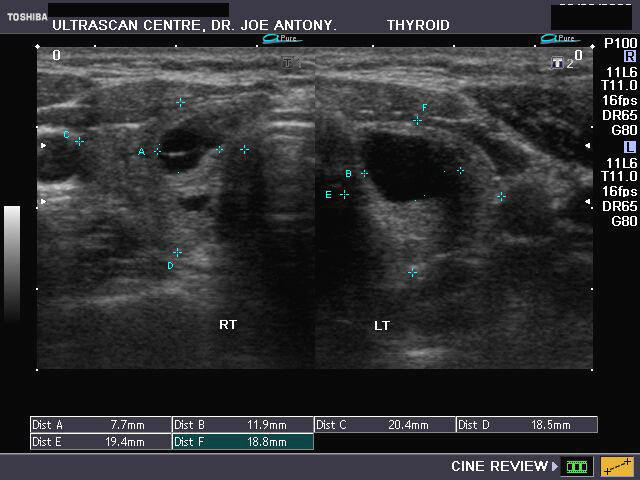
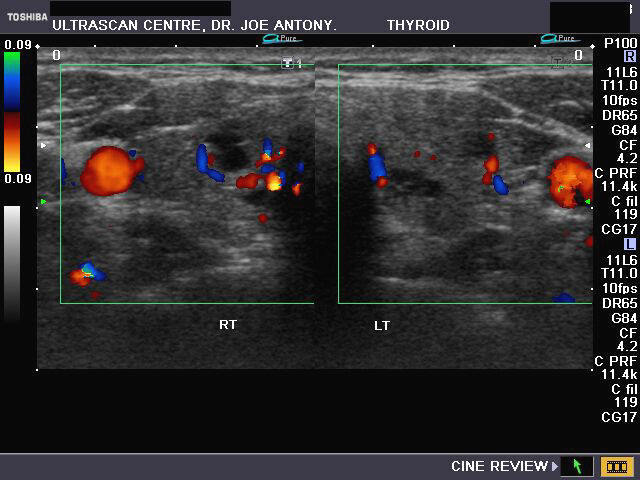
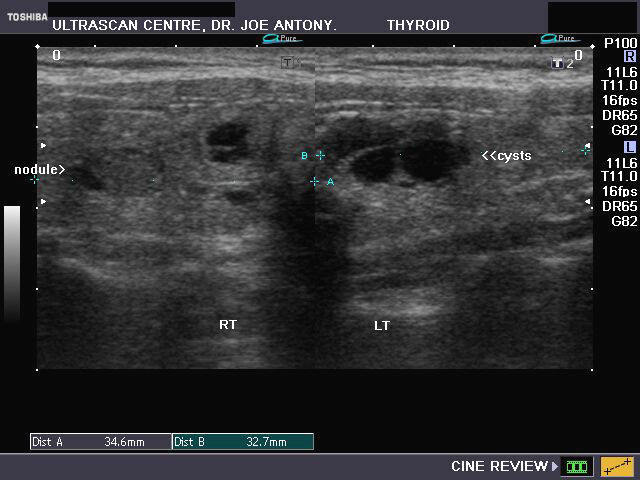
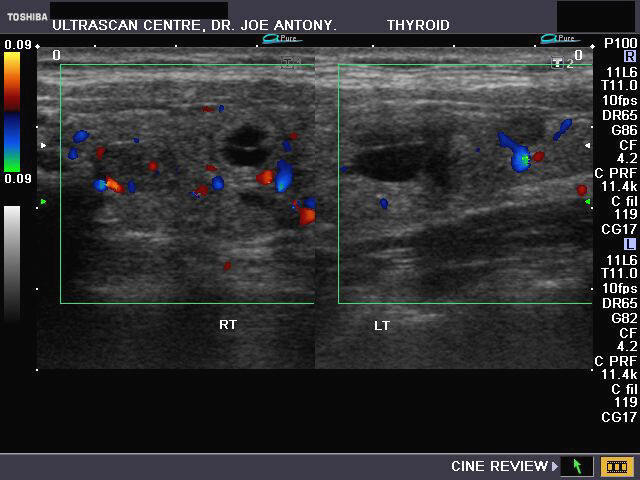
The above ultrasound and color doppler images reveal multiple cystic lesions in both lobes of the thyroid. There is also evidence of few nodular, solid masses within the lobes. Color doppler imaging reveals multiple vessels around the lesions. These images suggest multinodular goiter, more of a cystic variety.
Sublingual thyroid

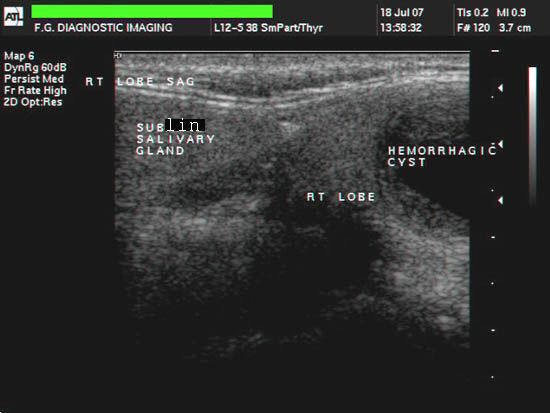
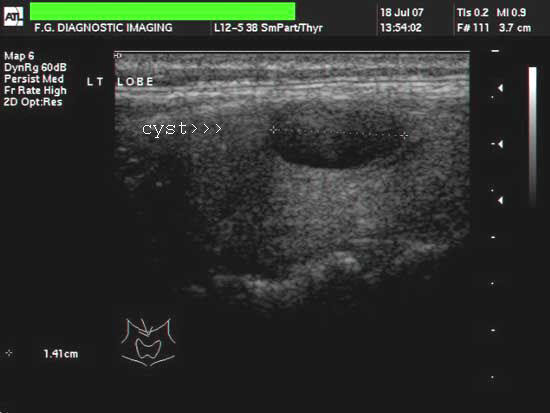
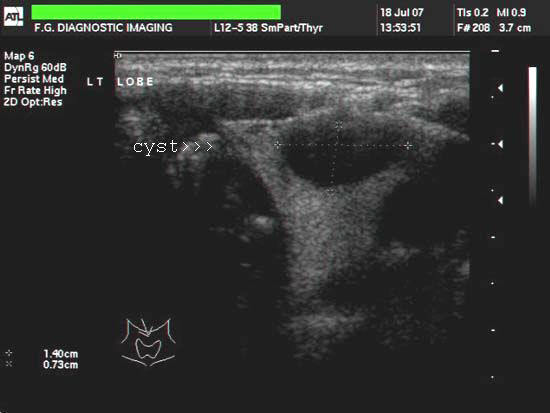
This young lady had a swelling in the right side of upper neck of acute onset. Ultrasound images of the neck reveal an extension of the right lobe of thyroid gland into the sublingual region of the neck. This showed a thick-walled cyst with thickened septae within it. The left lobe of thyroid also shows a simple colloid adenoma (cyst) within it. These ultrasound images suggest hemorrhagic cyst of sublingual thyroid. Images taken with an ATL ultrasound machine courtesy of Mr. Shlomo Gobi, Israel.
Reference:
1) http://www.ajnr.org/cgi/reprint/16/5/1117.pdf (free article)
2) http://jcem.endojournals.org/cgi/content/full/88/11/5145(free article and images)
3) http://pediatrics.aappublications.org/cgi/content/abstract/38/4/647 (abstract)
Ultrasound image of hemithyroidectomy
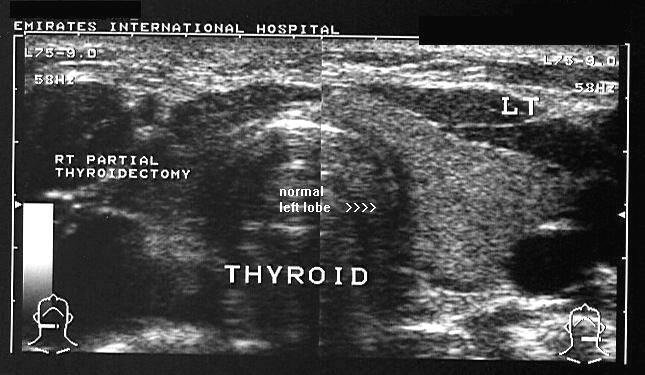
This sonographic image shows a post-surgical absence of the right half of the thyroid gland. Hemithyrodiectomy is usually done in cases of suspected thyroid malignancy. Here the normal left half of the thyroid is seen in transverse section. Ultrasound image taken with a Toshiba Powervision color doppler/ ultrasound machine, courtesy of Dr. Ravi Kadasne, MD, UAE.
Reference: Thyroidectomy article
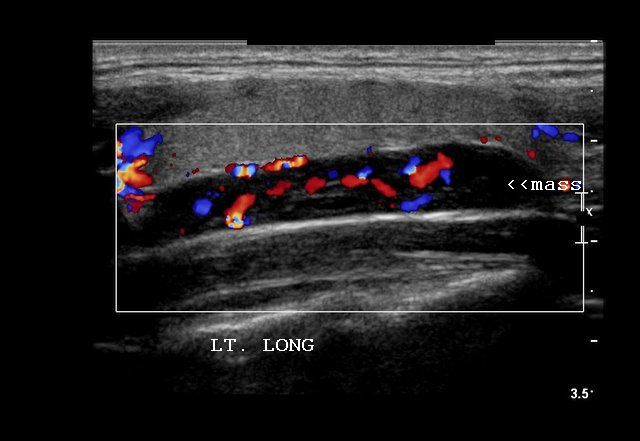
Superficial neck masses- lipoma
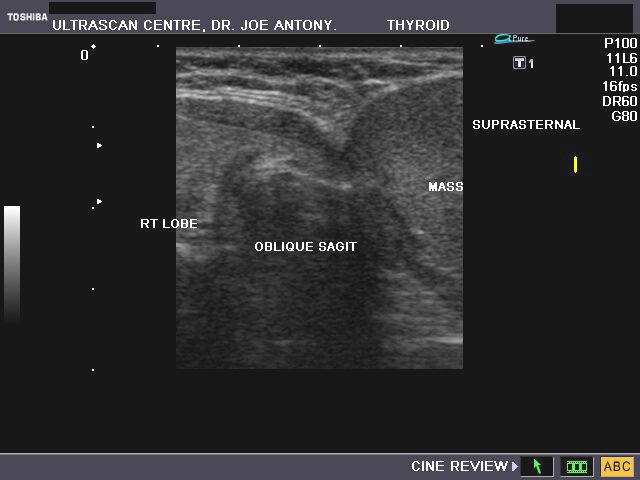
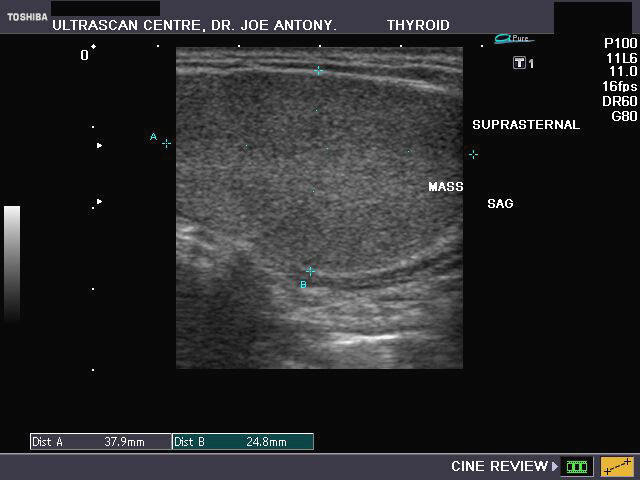
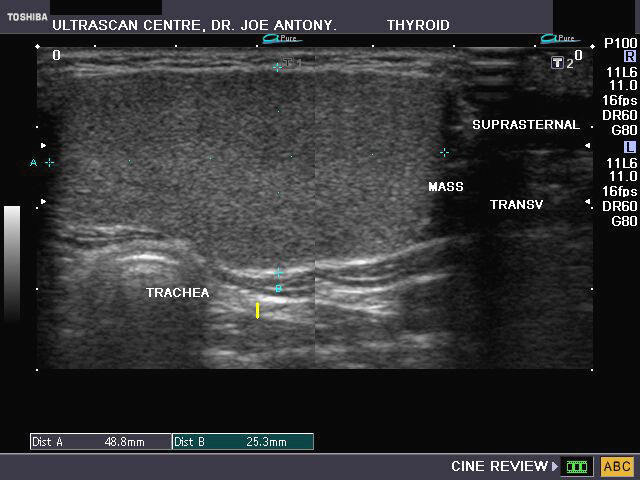


The normal thyroid is visualized above the mass, though small in size.
This teenaged female presented with a palpable and visible mass in the suprasternal region just below the thyroid. On sonography, the mass is homogenous in echotexture, measures 5.5 x 2.5 x 2.6 cms., relatively hyperechoic with echogenicity just less than the normal thyroid (which was well visualized). Color doppler imaging shows no vascularity in the mass. These ultrasound images suggest either an ectopic thymic mass or a subcutanous mass like lipoma. The mass was aspirated and proved to be a lipoma of the neck. Images taken using a Toshiba Nemio XG by Joe Antony, MD, India.
Reference: http://www.ajnr.org/cgi/reprint/19/3/505(an excellent free article and images).
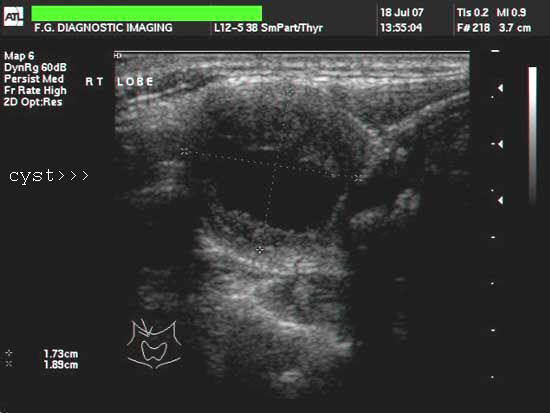
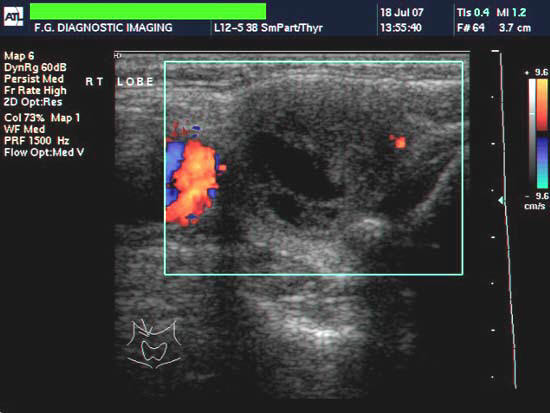
Hemorrhagic colloid cyst of the thyroid


The above sonographic images of the right lobe of thyroid show a large cyst measuring 1.8 x 1.5 cms. The walls appear irregular with fine debris within the lumen of the thyroid cyst. Color doppler image (on right) shows normal vascularity with no vessels within the cyst. These ultrasound images suggest Hemorrhagic colloid cyst of the thyroid.
Reference: http://www.emedicine.com/Radio/topic695.htm
Follow up ultrasound images (same patient above) 2 months later


The colloid cyst, has almost completely resolved and measures 0.8 cms. in size. Such dramatic improvement and reduction is known to occur in colloid cyst of the thyroid, especially if hemorrhagic in nature.
Malignant thyroid nodule
Case-1
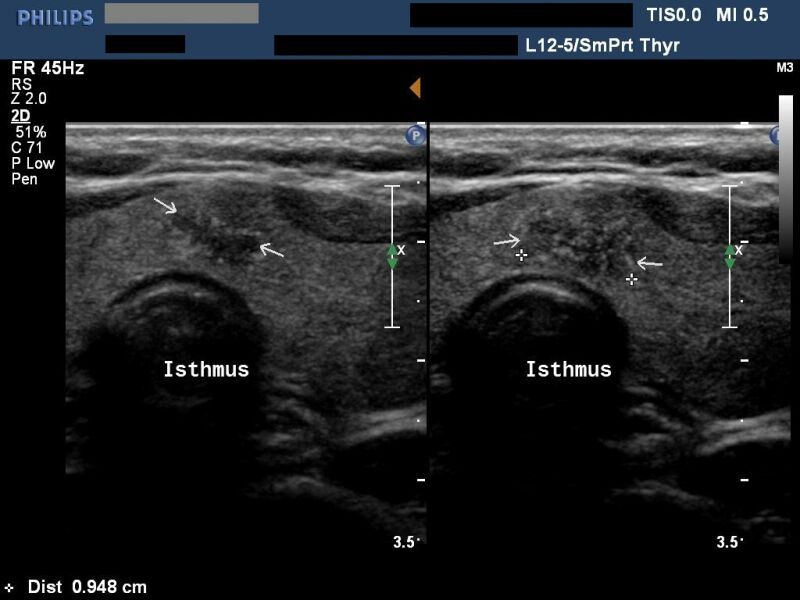

This patient underwent sonography of the thyroid, revealing a markedly hypoechoic nodule of 1.1 cms. width, in the left half of the isthmus of the thyroid. The lesion also shows echogenic specks s/o microcalcification and an irregular border. Also note that the nodule is as tall as it is wide. All these ultrasound findings favor a diagnosis of malignancy on this thyroid nodule. Images courtesy of Dr. Ravi Kadasne, UAE.
Reference:http://www.ajronline.org/cgi/reprint/178/3/687.pdf(excellent article-- free)
Case-2: Papillary carcinoma of thyroid- Left lobe


Left lobe- long section Left lobe nodule-long section- color Doppler- Transverse section of thyroid
This was a patient with a biopsy proven case of papillary carcinoma of the left lobe. The large hypoechoic mass is seen infiltrating large portions of the left lobe. No definite evidence of microcalcifications is seen. However color Doppler ultrasound shows marked increase in color flow within the affected part of the left lobe. The margins of the tumor appear poorly defined with absence of a clear hypoechoic halo around the mass. These ultrasound images of papillary carcinoma of the thyroid gland are courtesy of Dr. Ravi Kadasne, MD, UAE. Malignant masses of the thyroid are relatively rare and malignant transformation of thyroid nodules occur in as low as 7 % of nodules. Among thyroid malignancies, the commonest is papillary carcinoma and this variety of carcinoma has the best prognosis. The other forms of thyroid carcinoma are follicular, medullary and anaplastic. Of these the anaplastic carcinoma of the thyroid carries the highest mortality rate with a 5 year survival rate of less than 5 %. Papillary carcinoma of the thyroid has a 20 year survival rate of 95 %.
Case-3: Biopsy proven papillary carcinoma of thyroid- Right lobe
Right lobe mass with microcalcifications



This was yet another case of proven papillary carcinoma of the thyroid of the right lobe. The ultrasound images show a large, inhomogenous, hypoechoic mass of the right lobe with multiple calcific foci (microcalcifications). The ultrasound findings are confirmed by 3D sonography of the lesion which shows the calcific foci in clear contrast. Color Doppler image of the right lobe (long section) shows marked increase in internal vascularity of the nodule. Ultrasound images of this case of papillary carcinoma of thyroid are courtesy of Dr. Ravi Kadasne, MD, UAE.
Case-4: Biopsy proven medullary carcinoma of thyroid



B-mode ultrasound images of the mass in right lobe The upper pole shows a beingn colloid nodule
Right lobe thyroid with hypoechoic nodule and coarse, large calcification. Marked vascularity with chaotic vessels seen in the hypoechoic mass in the lower half of the right lobe.This middle aged (50 year old) female patient showed a markedly hypoechoic but solid mass in the lower half of the right lobe (1.2 x 1.5 cms.) with coarse calcification. This is a typical finding in ultrasound imaging of medullary carcinoma of the thyroid. Medullary carcinoma is typically seen in middle aged female patients. The marked vascularity of the lesion and chaotic vessels in the tumor are also suggestive of a malignant mass (in this case- medullary carcinoma) of the thyroid. Thyroid medullary caricnoma can metastatize to lymph nodes producing hypoechoic nodes. Usually the upper part of the thyroid lobe is affected in medullary carcinoma. Histopathological study confirmed this tumor to be medullary carcinoma. There is also a colloid nodule of the upper part of the right lobe.
References:
Ultrasound imaging of thyroid malignancy: http://radiographics.rsna.org/content/27/3/847.full
Benign nodules of the thyroid
a) Follicular adenoma
Case-1

Sonography of the thyroid was done in this young girl. There is a large, solid, echogenic, homogenous oval nodule with a hypoechoic halo around the lesion, in the right lobe of thyroid. The lesion is solitary, shows no cystic areas and has a rim of vessels entering it's central area. These ultrasound images are diagnostic of a benign follicular adenoma of the thyroid. Note the similarity of the egg-shaped lesion to a sonographic image of the testes.
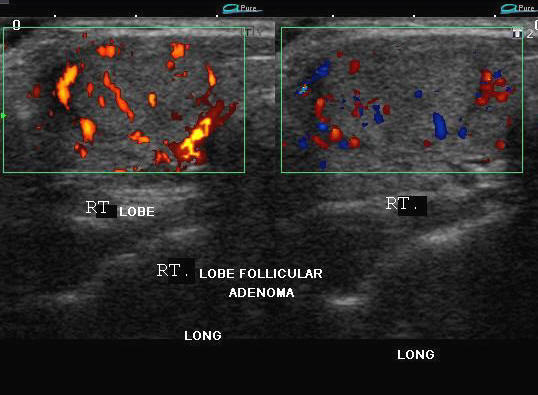
Case-2: Large Follicular adenoma of right lobe of thyroid


This 30 yr. old female patient has a right sided thyroid nodule. The nodule moved with deglutition and seemed to occupy a large part of the right lobe. Ultrasound images show a solid, egg-shaped mass which has features similar to the previous case-1 (above). However, this thyroid nodule is much larger (at 4 x 1.5 cms.). Note the absence of cysts or calcification within the thyroid nodule. These ultrasound appearances are typical of right follicular adenoma of the thyroid. The main differential diagnosis in this case is adenomatous nodule of the thyroid. However, as mentioned, the homogenous appearance, absence of cysts and solitary nature of this nodule are in favor of a follicular adenoma.
b) Adenomatous nodules
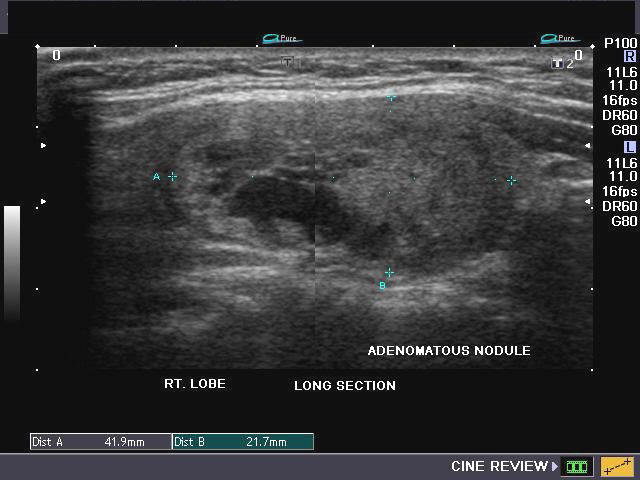
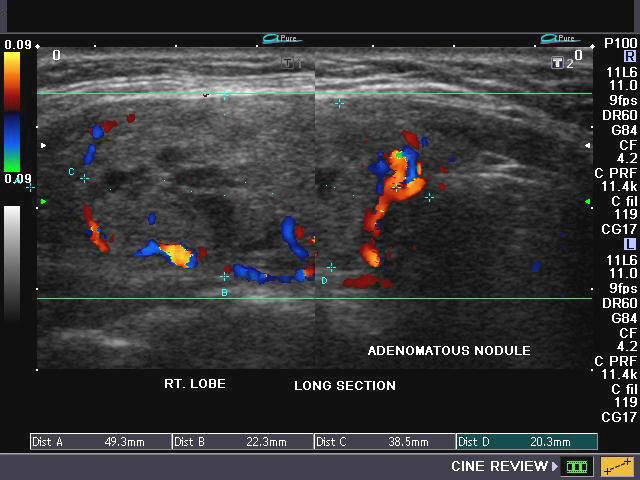
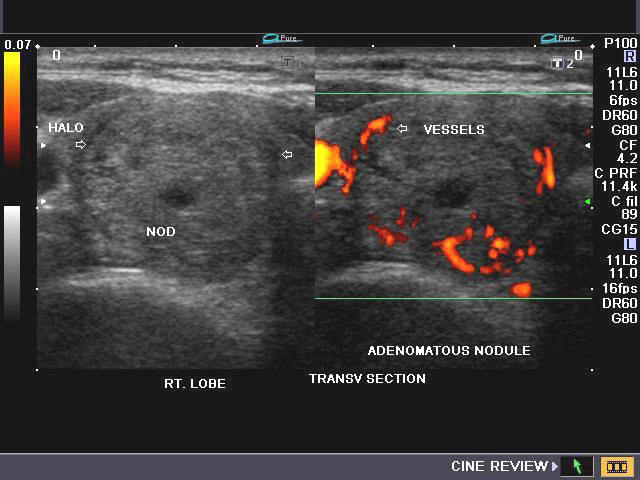


Both the above cases (1 and 2) show large, well-defined complex masses in the thyroid gland. In case 1 the masses are multiple. Both patients show multiple vessels along the rim of the masses and have cystic areas in a primarily solid mass. Unlike follicular adenoma, the masses are inhomogenous and multiple. Few intranodular vessels are present. There is a poorly defined halo (marginal hypoechoic rim) in these lesions. These ultrasound features/ images are highly suggestive of adenomatous or colloid nodules of the thyroid gland. The vast majority of thyroid nodules fall in this category.
Reference: http://emedicine.medscape.com/article/385301-overview(free article and images).
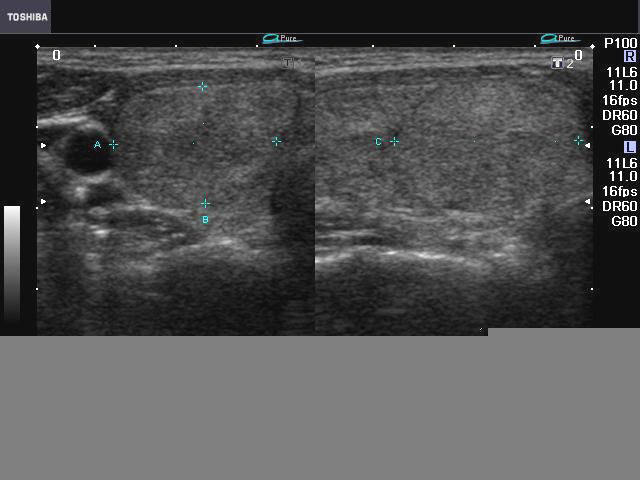
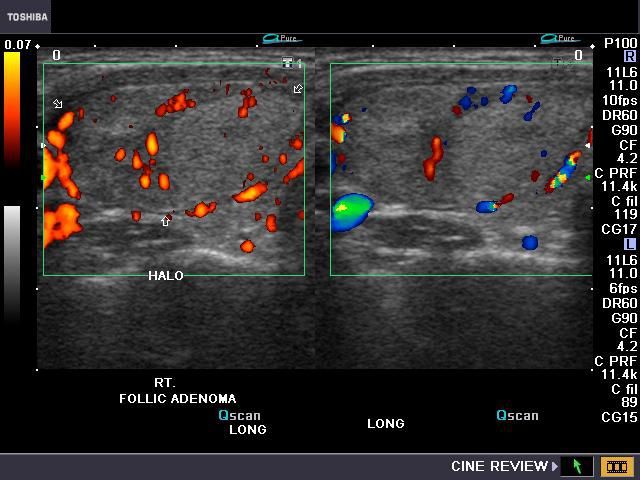
follicular-adenoma-case-3

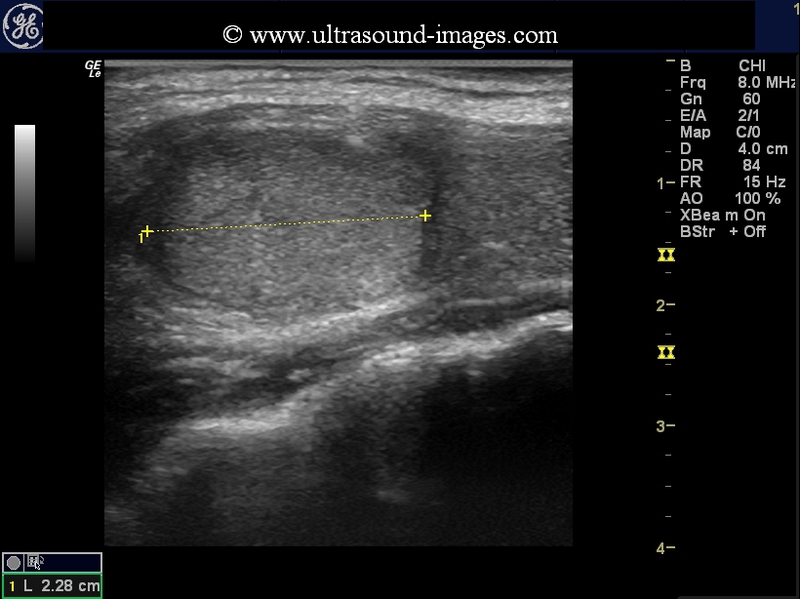
This is another case of follicular adenoma of the right lobe of thyroid. Ultrasound images show similar features as the above 2 cases of follicular adenoma. However, a small hypoechoic lesion is also present in this nodule. The presence of a hypoechoic lesion in a case of follicular adenoma should also prompt further investigation including FNAC and follow up ultrasound. It must be emphasized that it is almost impossible to differentiate a follicular adenoma from a malignant version of the same neoplasm (name follicular carcinoma of the thyroid). However, features suggesting obvious malignancy are markedly hypoechoic areas with increased vascularity. Medical literature states that even a FNAC may often be unable to correctly sample tha site of potential carcinoma within a pre-existing follicular adenoma (note that most follicular carcinomas develop as a result of malignant transformation within a benign follicular adenoma).
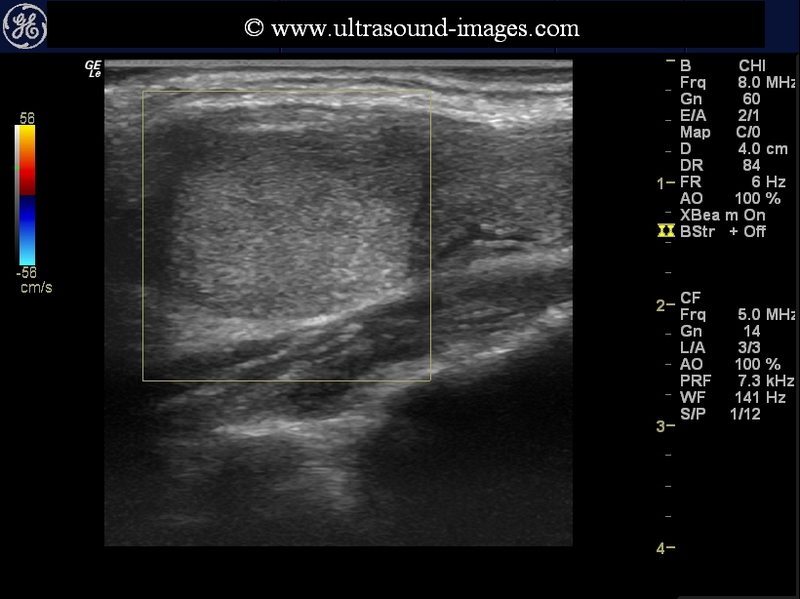
The 3rd image (extreme right- above) shows a color Doppler study of the nodule but in this there is no Doppler flow signal seen because the Doppler PRF settings are raised high enough to prevent it. This technique is useful in imaging the nodule for microcalcification which may not be seen on ordinary B-mode ultrasound imaging of the thyroid. In this case, even with this method there is no evidence of microcalcification seen.
Case-3: Adenomatous or colloid nodule of left lobe- 3D ultrasound and elastogram
A large colloid or adenomatous nodule is present in the left lobe. It shows a complex internal structure
B- mode image- long section


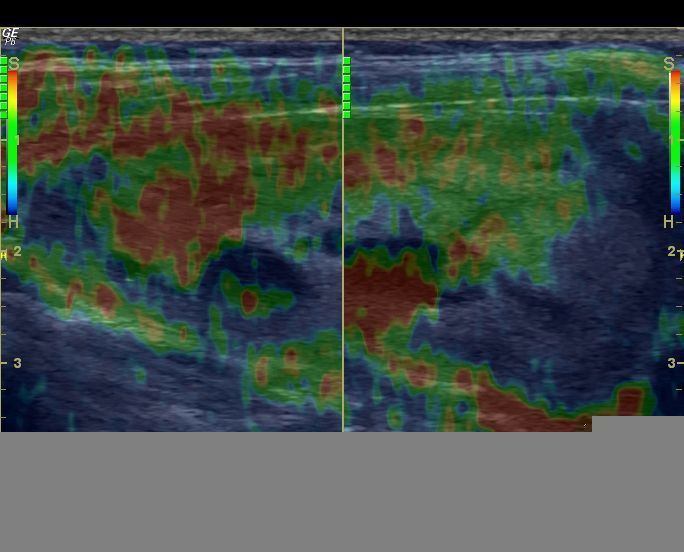
The red and green areas suggest soft tissue in the nodule which occupies the entire left lobe. The blue regions in the mass suggest potential malignant changes due to brittle or hard tissue.
3D ultrasound images of the left lobe mass
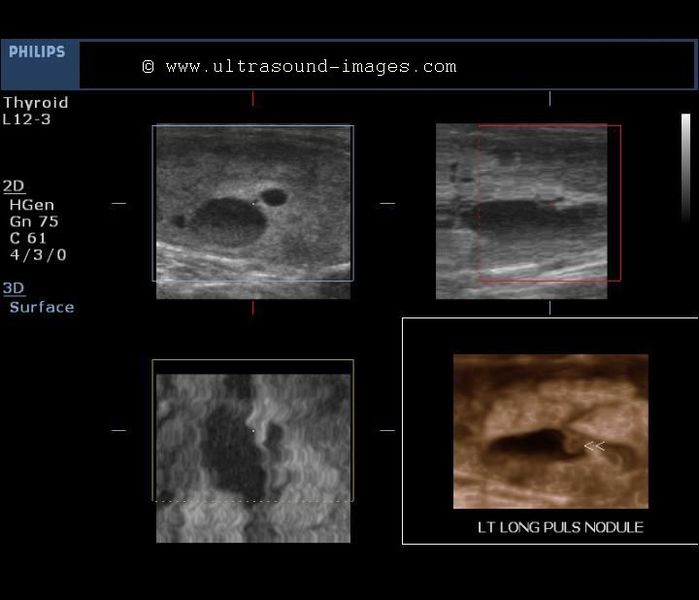
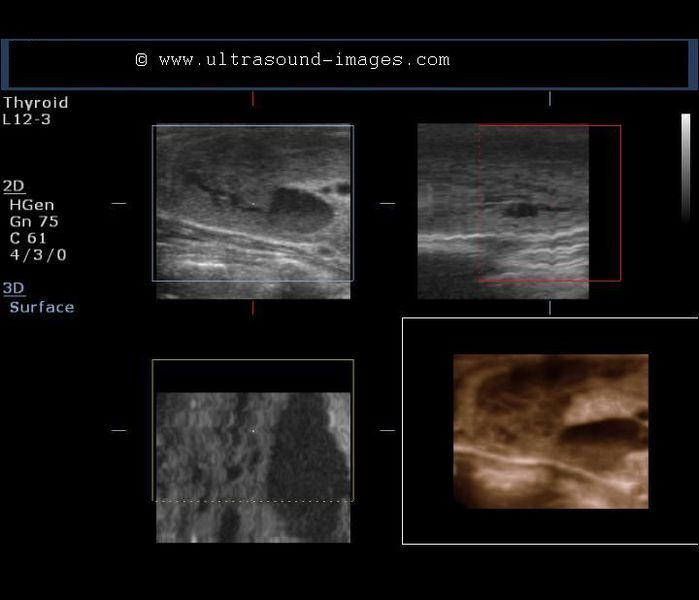
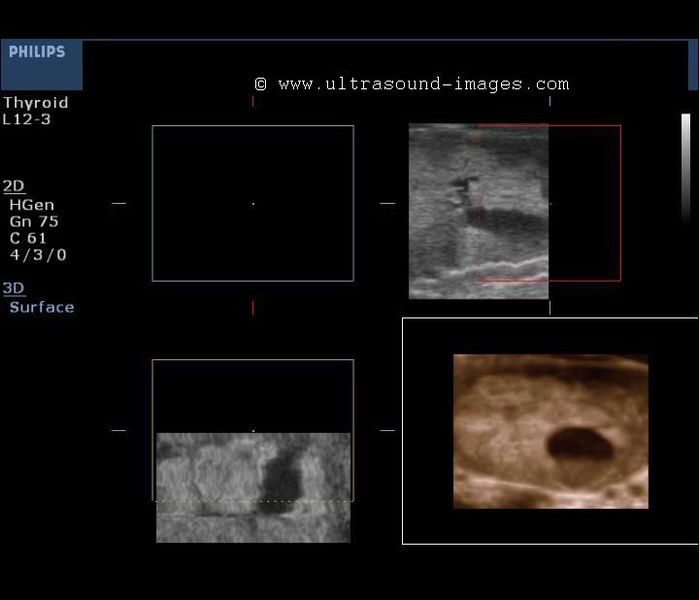
Note the details of the mass in the left lobe with the cystic area of the mass shown clearly. There is a mural nodule in the cystic area. Also note the presence of fluid debris layering suggesting particulate matter in the cystic area. 3D ultrasound images of adenomatous nodule were taken with Philips HD 15 ultrasound machine. The Elastogram of the thyroid was done using a GE P6 pro ultrasound system.
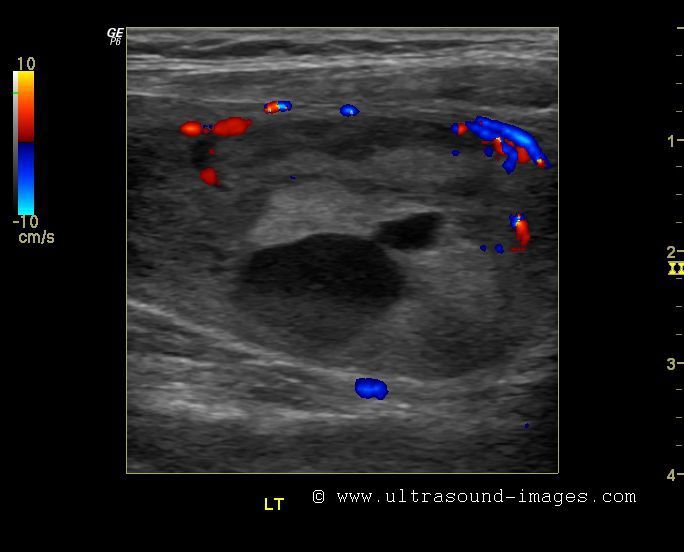
Toxic thyroid nodule
Large solid, colloid nodule is seen in right lobe




Spectral Doppler waveform shows marked increase in PSV of the vessels in right lobe (50 cms./sec) as compared to the PSV of the vessels of normal left lobe (20 cms./sec):
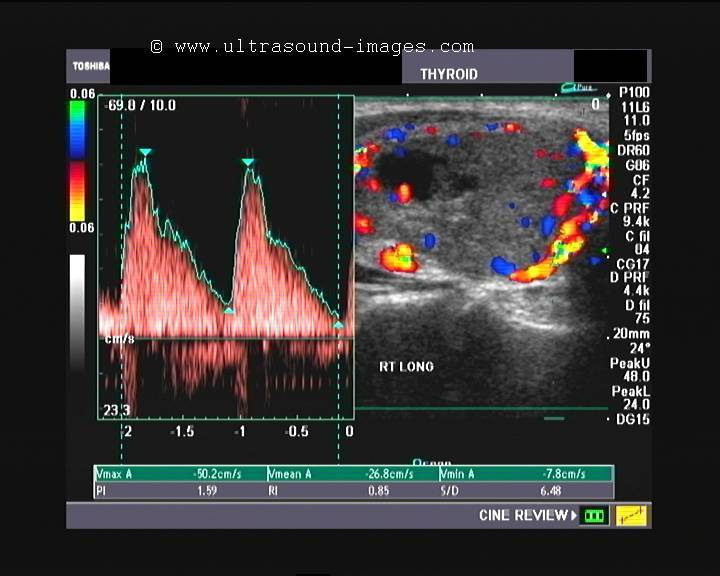

A markedly vascular right thyroid colloid nodule with high Peak systolic velocity (PSV) of the arterial flow in the right lobe is indicative of a possible toxic nodule. Normal PSV of the superior or inferior thyroid arteries is less than 18 cms./sec. In thyrotoxicosis, the PSV can reach from 20 to 120 cms./sec or even higher. This patient was a middle aged female with h/o of loss of weight and heat intolerance.
Ectopic thyroid tissue




This young female patient has an ectopic thyroid nodule just above the thyroid cartilage with co-existing (orthotopic) thyroid in the normal thyroid fossa. The ectopic thyroid nodule shows solid tissue and is possibly functional. However, it may be surgically removed, if needed, as functional thyroid tissue is seen in normal location. The orthotopic thyroid gland shows changes of Hashimoto's thyroiditis.
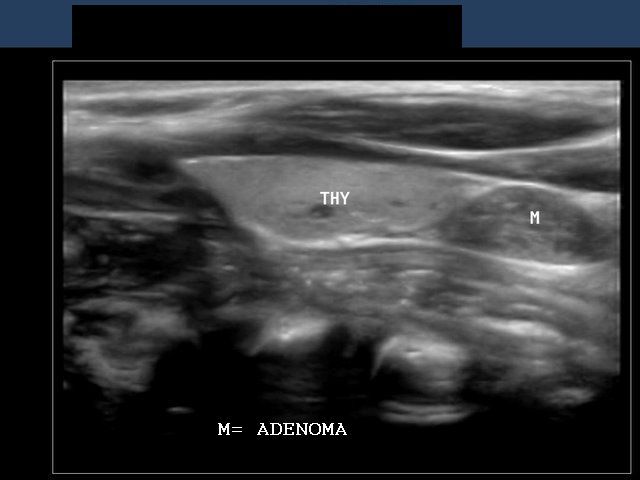
Parathyroid adenoma
Adenoma of the parathyroid gland


The parathyroid glands are located posterior to both lobes of the thyroid gland are 4 in number, the superior and inferior pairs. The parathyroid glands regulate the metabolism of calcium in the body and parathyroid hormone (PTH) causes increase in calcium level in the blood. The commonest cause of Hyperparathyroidism is parathyroid adenoma. Sonography of the parathyroid glands (above) shows a markedly hypoechoic, oval mass seen posterior to the left lobe of thyroid. These ultrasound images are suggestive of parathyroid adenoma. Both above images of parathyroid adenoma are courtesy of Dr. Durr E Sabih, Pakistan.
Reference:http://emedicine.medscape.com/article/384024-overview (free article and images)
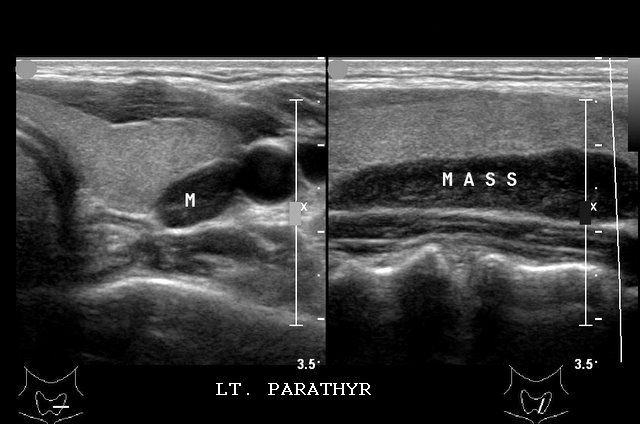
Case-2 : Parathyroid adenoma in child
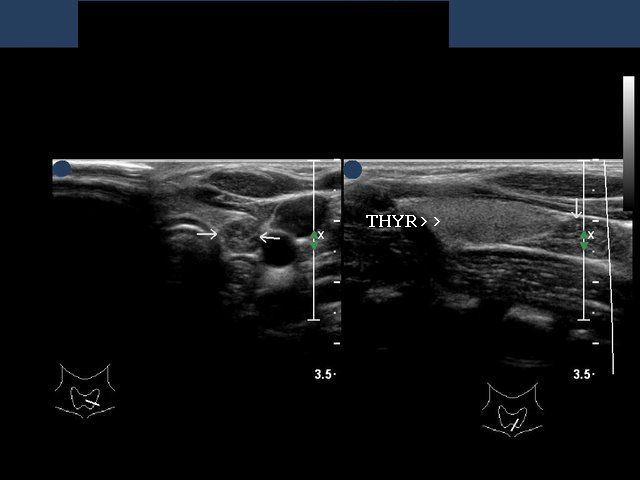
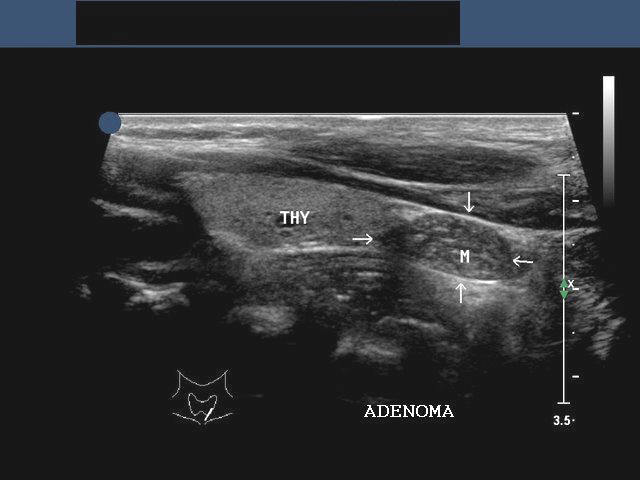
This was a 9 yr. old female child with hypercalcemia and nephrolithiasis. Ultrasound imaging of the left thyroid and parathyroids show a hypoechoic mass in the region posterior to the lower pole of left lobe of thyroid (similar location as in case-1). The image in bottom row is a 3-D ultrasound image of the parathyroid adenoma. (THYR= thyroid, left lobe). All sections are oblique longitudinal views of the lesion seen via the left lobe of thyroid gland. Images are courtesy of Ravi Kadasne, MD, UAE.
Another case of Parathyroid adenoma (case-3)



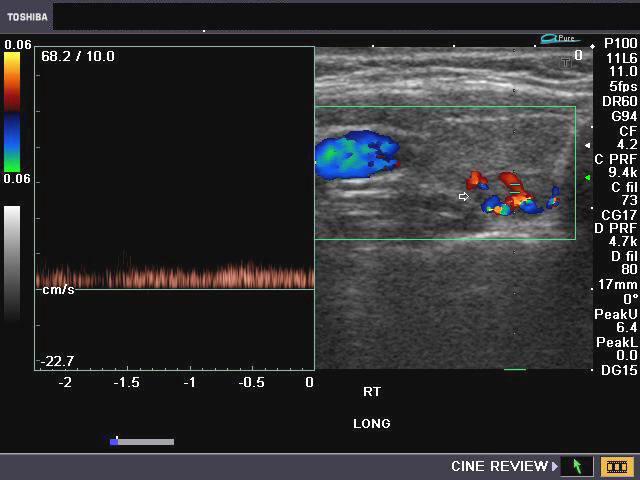

This was a middle aged female patient with suspected thyroid pathology. Ultrasound images show a relatively large, well encapsulated hypoechoic mass of 1.1 x 0.5 cms. in the posterior aspect of the right lobe of thyroid. The main differential diagnosis in this case is a parathyroid adenoma (right -lower). The color Doppler images show marked vascularity with an arc of vessels around the lesion. This is a highly suggestive sign of parathyroid adenoma. The other main differential diagnosis is "hot" autonomous nodule of the thyroid gland (less likely). The vessels show both arterial and venous flow within this lesion.
Reference:http://www.jultrasoundmed.org/cgi/content/abstract/13/4/303)
Case-4: Huge parathyroid adenoma

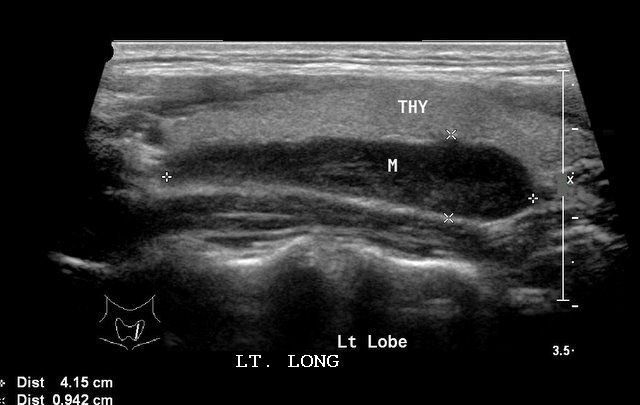
This is a huge left parathyroid adenoma. Again the mass is typical in location, and markedly hypoechoic. However, the size is an astonishing 4.2 x 1 cms., one of the largest I have seen. The long section shows its elongated nature, extending along (posterior to) the length of the left lobe of thyroid. Ultrasound images are courtesy of Dr. Ravi Kadasne, MD, UAE. The color Doppler image shows considerable vascularity in the parathyroid mass.
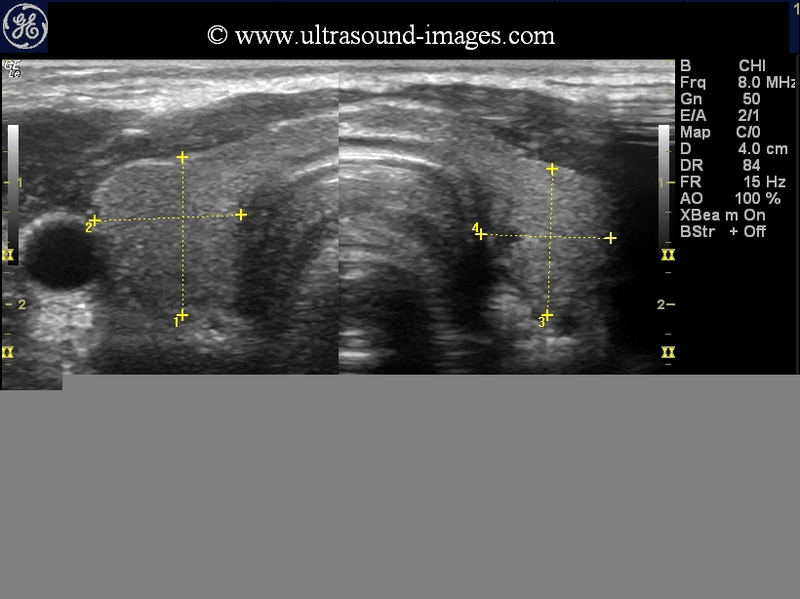
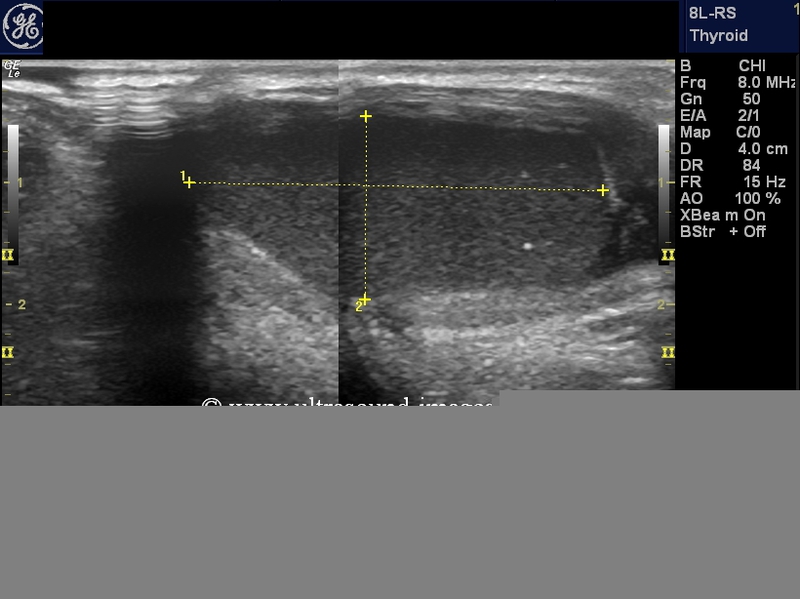
Thyroglossal duct cyst




p>This 4 year old male child showed a gradually increasing swelling just left of the midline (see snaps above). Sonography of the neck showed a normally located thyroid gland (see ultrasound image top- left) or orthotopic thyroid which was normal in structure and echogenicity. However, the ultrasound image on right shows the cystic mass seen in the photos in lower row. The cyst is well defined and has no significant vessels in its walls. The cyst shows clear fluid content and no septae or nodules. These findings favor a diagnosis of thyroglossal duct cyst. Thyroglossal duct cysts though usually seen in the midline, may be located, slightly on one side (here just left of the midline). The cyst showed movement with deglutition. Surgery would be an ideal option in this case, as the thyroglossal duct cyst does not contain functioning thyroid tissue; besides, the child has a normal orthotopic thyroid gland.
thyroglossal-duct-cyst-case-2


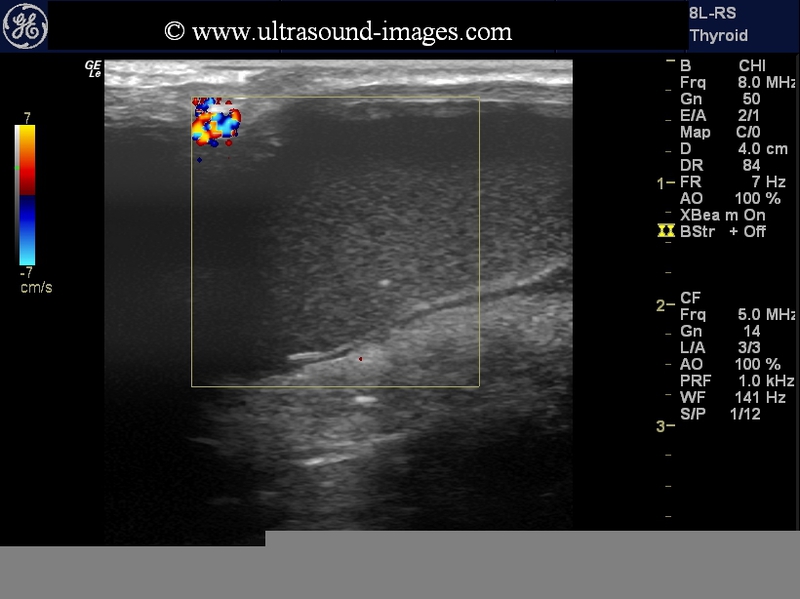
This midline mass was clinically seen to move with deglutition and was located just lateral to (the left of) midline in this young adult male. The patient did not complain of pain or tenderness in this region though pressure effect produced some irritiation and discomfort whilst swallowing. Ultrasound images show the orthotopically located thyroid in the thyroid fossa which did not show any abnormality. However, the midline swelling shows echogenic homogenous debris or particulate matter that did not show evidence of motion on probe movement. This suggests that the lesion is a large cystic mass containing protein like or colloid or jelly like matter which is one of the presentations of a thyroglossal duct cyst. Color Doppler ultrasound further confirmed that this lesion is not vascular nor showed rim vascularity ruling out infective pathology.
Final diagnosis: colloid matter within a thyroglossal duct cyst.
Thyroglossal duct cyst inflammation/ abscess


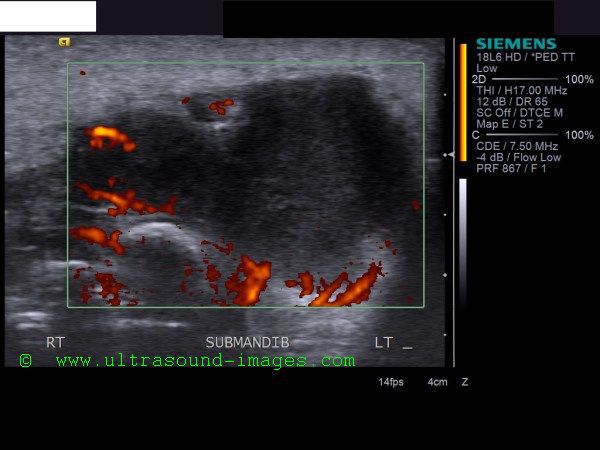



This new born baby had a swelling and tenderness over the lower submandibular region/ chin. Ultrasound images of this region showed a midline hypoechoic region with fine echoes within it. The margins of the cystic lesion appear thick-walled and irregular. Power Doppler image (lower left), shows considerable vascularity around the walls of the cyst suggesting inflammation. The cyst measures 2.4 x 1.7 cms. in size, and shows no septae. The midline location of this cystic mass suggests possibility of thyroglossal duct cyst, with the other ultrasound findings suggesting inflammation or abscess formation. Thyroglossal duct cysts are the commonest cause of neck and chin swellings in the neonate/ newborn. Inflammation following infection of the thyroglossal duct cyst is a common and known complication of this lesion. Thyroglossal duct cysts may be suprahyoid (above the hyoid cartilage), as in this case, hyoid level, or infrahyoid in location. They may be midline (usually) or just to the side of the midline. Below are some snaps of the neonate's chin. This case and ultrasound images of thyroglossal duct cyst abscess are courtesy of Mr. Shlomo Gobi, sonographer, Israel.
Reference: http://www.jultrasoundmed.org/cgi/reprint/27/8/1211
Branchial cleft cyst or Branchial cyst
B-mode ultrasound image-Rt. Branchial cyst
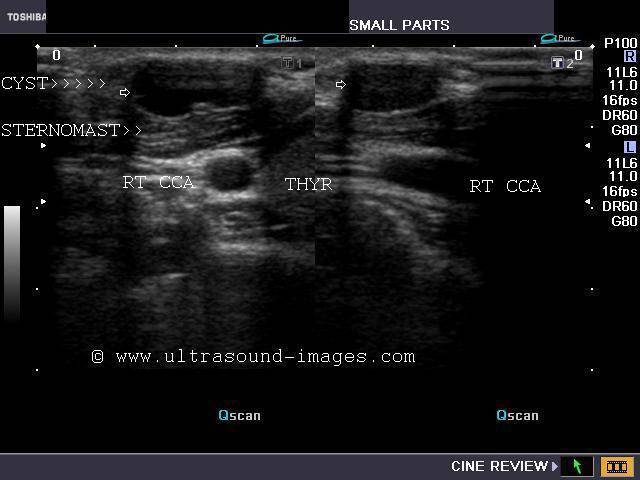
Relation of the Branchial cyst to CCA seen in
Rt. lobe of thyroid and Sternomastoid muscle


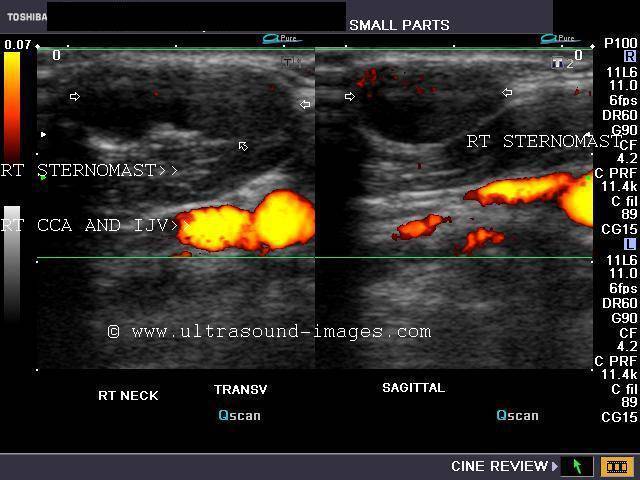
This young lady presented with a soft painless swelling of the right anterior triangle present since birth. Ultrasound images show an aseptate cystic lesion of 2 x 1 cms. in the anterior triangle of the right side of neck, superficial to the anterior border of the sternomastoid and just lateral to the right lobe of thyroid. This is the typical ultrasound appearance of a Branchial cleft cyst or Branchial cyst. The cyst is separated from the deeper common carotid artery and Internal jugular vein by the right sternomastoid muscle. Among congenital cysts the commonest cause of lateral neck swellings are branchial cleft cysts. There are 4 subtypes of branchial cysts. Of these the commonest is the 2nd branchial cleft cyst. The lesion described in the case study above appears to be of this subtype (i.e.- 2nd branchial cleft cyst).
Differential diagnosis:
The lesion is to be differentiated from cystic hygroma, another cystic swelling of the neck. Cystic hygromas arise due to dilatation of the lymph vessels (lymphangiomas) and are classically thin walled and multi-septate. Besides, cystic hygromas are closely related and usually surround the neurovascular bundles of the neck. Thyroglossal duct cysts arise from the thyroglossal duct and move with swallowing. Thyroglossal duct cysts are usually midline in location. The other lesion that may mimic branchial cysts are necrotic lymph nodes, usually post tubercular infections. The history is crucial here.
References:
2) Sonography of branchial cleft cysts
Sonographic atlas of the thyroid
Do you wish to read more on ultrasound imaging of the thyroid?
I have published a short easy to read book on sonography of the thyroid, printed and distributed world wide by Jaypee brothers, India. Very inexpensive and easy to master, this short handbook uses the best ultrasound images of most thyroid diseases to explain the various pathology affecting the thyroid gland and its sonographic diagnosis. Sonography of the thyroid is perhaps one of the most affordable and safest method of studying thyroid diseases. My book:"Sonographic atlas of the thyroid and appendix" explains almost every thyroid condition the reader would encounter during his/ her ultrasound practice. I have added a short section on various appendicular pathologies and its ultrasound diagnosis. Both parts of this short atlas of the thyroid and appendix will help the reader master the sonography of thyroid diseases as well as expose him to different types of appendicular diseases.
This excellent book is available in Jaypee brothers book shops in India and can also be bought online from a number of dealers. Visit:
2) sonographic atlas of thyroid and appendix
3) Ultrasound atlas of thyroid and appendix
4) Sonography of the thyroid- Jaypee brothers website
5) http://www.bookshopofindia.com/search.asp?action1=default&bookid=9081727
6) http://www.maansu.com/9788184489989
7) Sonographic atlas of the thyroid and appendix- Amega books
8) http://www.flipkart.com/b/books/step-sonographic-atlas-thyroid-appendix-book-8184489986
Priced at very affordable rates, this text book on ultrasound imaging of the thyroid is a must buy for the novice sonographer as well as the professional who wish to know more about thyroid ultrasound.
© 2026, Joe Antony, MD All images and content in this site are copyrighted. www.ultrasound-images.com When visiting this site, we may use cookies to improve the performance of this site. Use of this site means you accept the use of cookies. Read our privacy policy at this page: https://www.ultrasound-images.com/privacy-policy/