
Gall bladder
Contents of this page
- Normal Anatomy of Gall bladder
- Normal anatomical variants of the gall bladder: The phrygian cap deformity
- Carcinoma of gall bladder
- Gall bladder duplication
- Mirizzi syndrome
- 3-D ultrasound imaging of gall bladder calculi
- Calculus in Hartmann's pouch of gall bladder
- Limy bile
- Gall bladder sludge
- Tumefactive gall bladder sludge
- Gall bladder sludge with layering
- Gall bladder sludge simulating gall bladder neoplasm or mass
- Cholangiocarcinoma of CBD (common bile duct)
- choledocholithiasis-CBD-calculus
Normal Anatomy of Gall bladder




The above ultrasound images show the normal anatomy of the gall bladder taken from different angles of the transducer during sonography. The parts seen here are the fundus, body, neck and the cystic duct. Note the close relation of the cystic duct to the portal vein. The cystic duct is well seen and appears tortuous in these images.
Normal anatomical variants of the gall bladder: The phrygian cap deformity

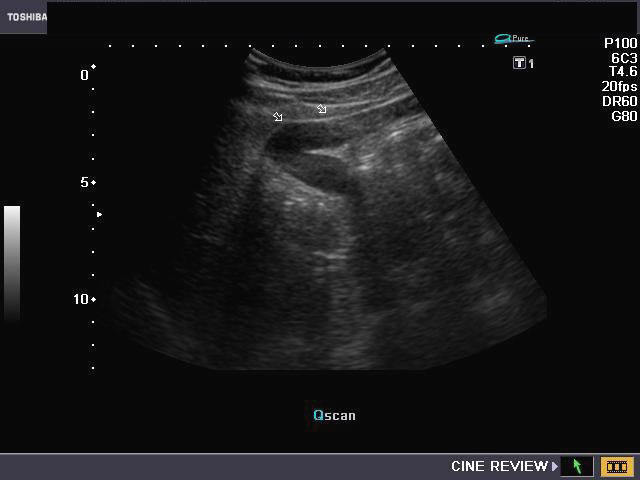
Variation in normal GB.
The gall bladder often folds on itself, at the junction of the fundus with body. (See snap of the phrygian cap)-- this results in a normal anatomical variant called the Phrygian cap gall bladder. This appearance can be mistaken by the sonologist with septate gall bladder. The above ultrasound images show the typical Phrygian cap gall bladder.
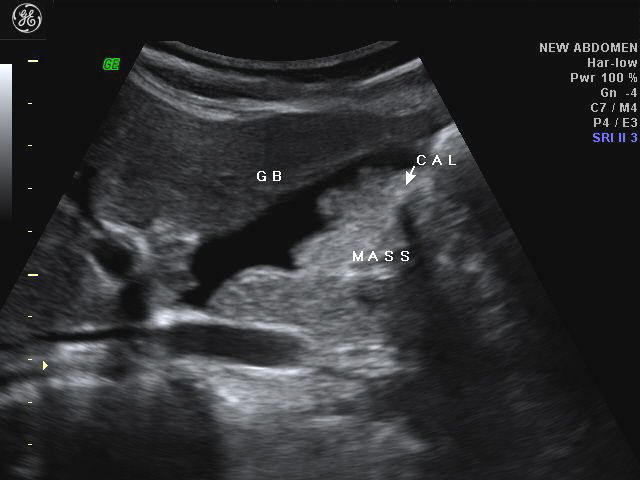
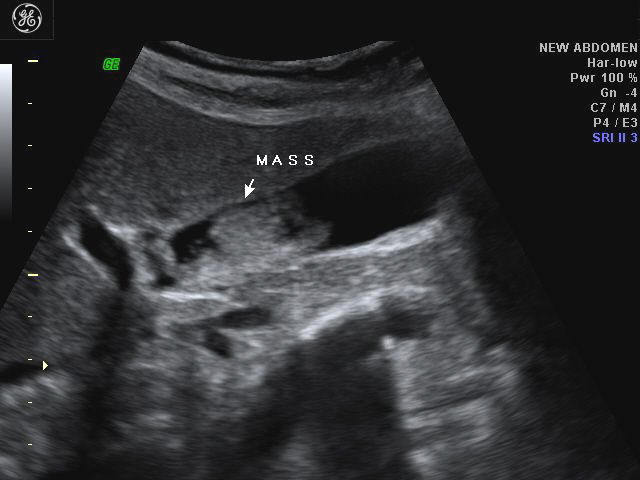
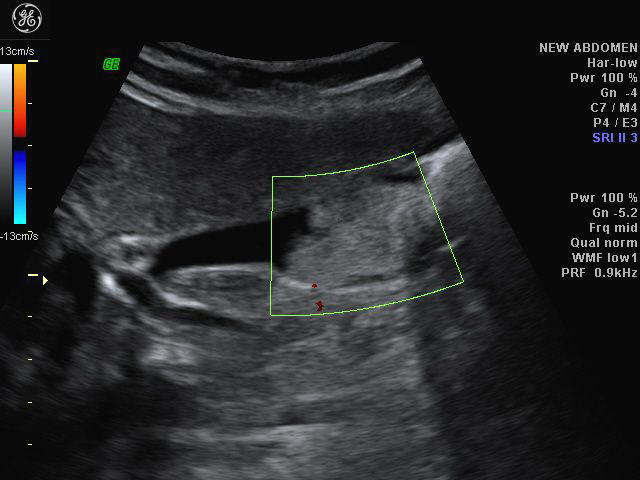
Carcinoma of gall bladder


This a middle aged male patient who presented with constipation. Ultrasound images of the liver and gall bladder reveal an ominous mass infiltrating the gall bladder wall with invasion of the right lobe of liver. There is also a large calculus seen in the gall bladder. These ultrasound images are diagnostic of gall bladder carcinoma. Images taken using a Toshiba Nemio 30 sonography machine, courtesy of Dr. Vikas Arora, Radiologist, Ferozepur, India.
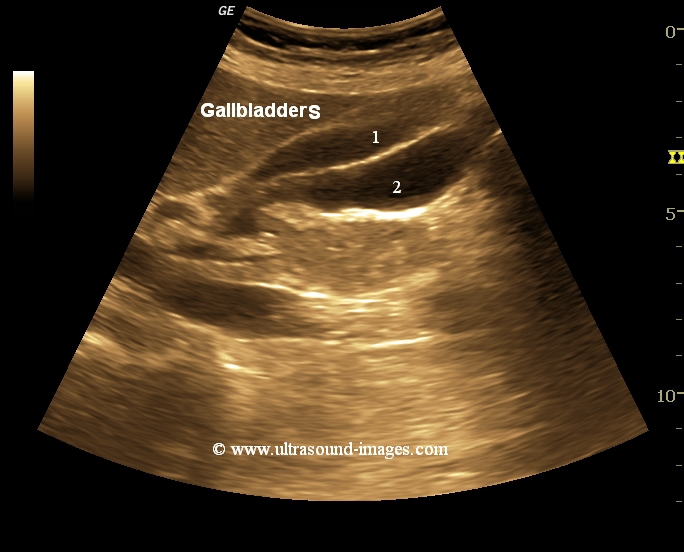
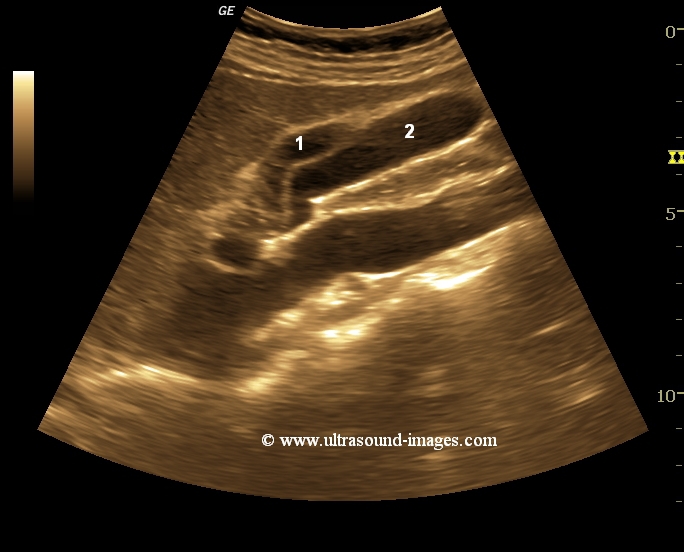
Gall bladder duplication






Ultrasound images of double gall bladder:
Abdominal sonography of a neonate revealed distended gall bladder with a similar, anechoic, tubular structure adjacent to it. Detailed examination revealed it to be a duplicate gall bladder. These ultrasound images of duplication of the gall bladder reveal 2 gall bladders adjacent to each other with 2 separate cystic ducts. After meals, both the gall bladders showed normal emptying. This is very rare, as it shows that both sacs are fully functional and connected to the Common bile duct (CBD). Images courtesy of Mr. Shlomo Gobi, Israel.
References:Journal of ultrasound article on gall bladder duplication
duplicate gallbladder with calculus- case-2
These 2-D and 3-D ultrasound images show a duplication of the gallbladder with a calculus lodged in the neck of one of the gallbladders. The presence of clear fluid (bile) within both the gallbladders suggests communication with the common bile duct. These 3-D ultrasound images of gallbladder duplication are courtesy of Dr. Sanjiv Bhalla.
Mirizzi syndrome



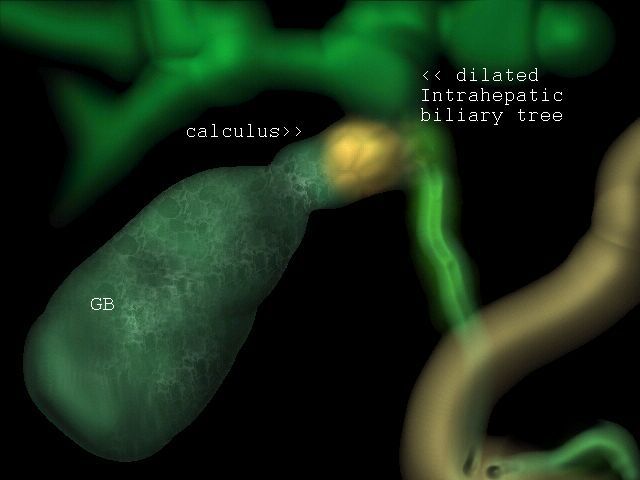
This patient presented with abdominal pain. Sonography reveals a well distended gall bladder with a stone in the neck of the gall bladder/ or cystic duct (see top). Ultrasound images of the liver reveal intrahepatic biliary tree dilatation, with a common bile duct (CBD) of normal calibre. Sonographic images of the liver give a false impression of the calculus being in the hepatic duct, due to the close proximity of the stone in the gall bladder neck. These ultrasound images are diagnostic of Mirizzi syndrome. This syndrome is caused by impacted calculus in the Gall bladder neck or cystic duct causing extrinsic compression of the common hepatic duct. A common predisposing factor for this is the low insertion of the cystic duct into the common hepatic duct. This makes the cystic duct almost parallel to the common hepatic duct. Ultrasound images are taken with a Toshiba Nemio 30 scanning machine, courtesy of Dr. Vikas Arora, Ferozepur, India. Artist's rendition of the syndrome courtesy of Dr. Anatoly Garkusha, Kiev, Ukraine.
Reference: http://www.emedicine.com/radio/topic451.htm(free article)
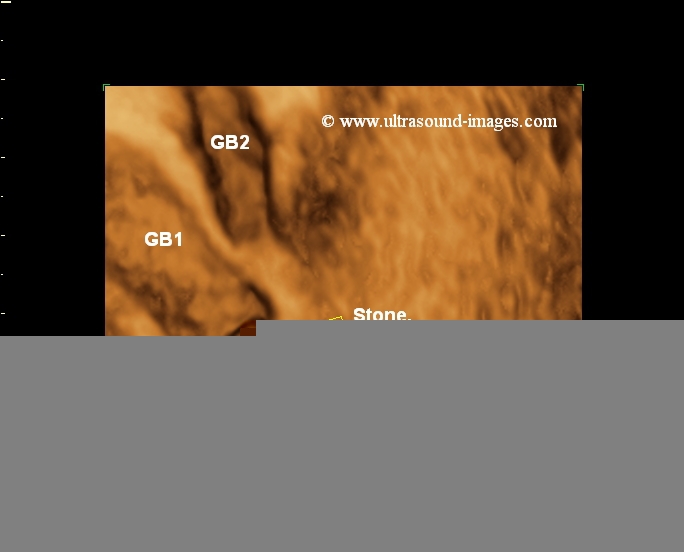
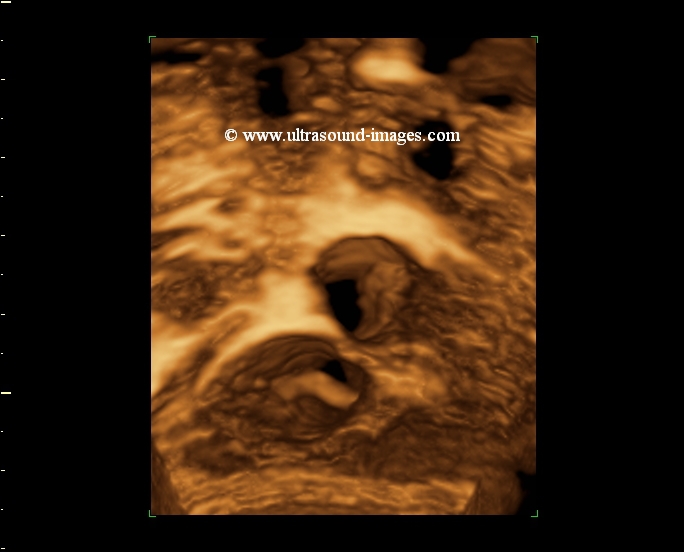
3-D ultrasound imaging of gall bladder calculi
This 3 Dimensional ultrasound image of the gall bladder shows multiple calculi in its lumen. Very often, it is difficult to be certain if a lesion is within the lumen or intramural. 3-D imaging helps in such cases. The amount of detail seen in such an image can also help plan management of the gall bladder calculi. Ultrasound image taken by Dr. Ravi Kadasne, UAE, using a Philips IU-22 ultrasound system.
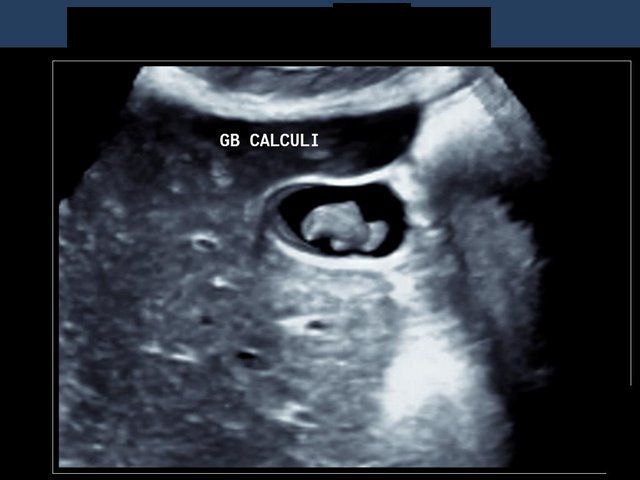
Calculus in Hartmann's pouch of gall bladder
Case-1
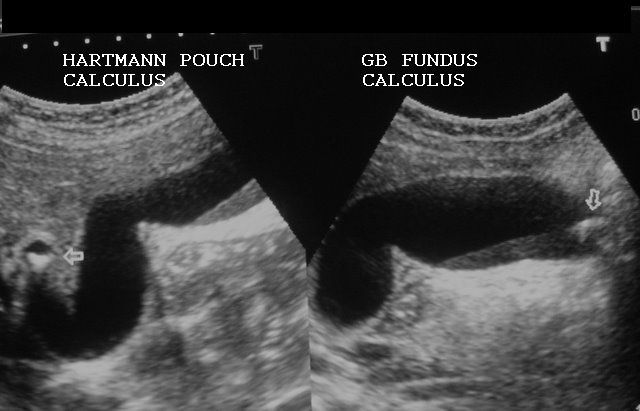

This patient presented with severe pain in the right hypochondrium. Sonography of the gall bladder shows a calculus impacted at the junction of the neck of GB (gall bladder) and the cystic duct (the pouch formed in this area is called the Hartmann's pouch). The gall bladder is hugely distended with another calculus seen in its fundus. Ultrasound images are courtesy of Dr. Vikas Arora, MD, India.
Case-2: Hartmann's pouch calculus
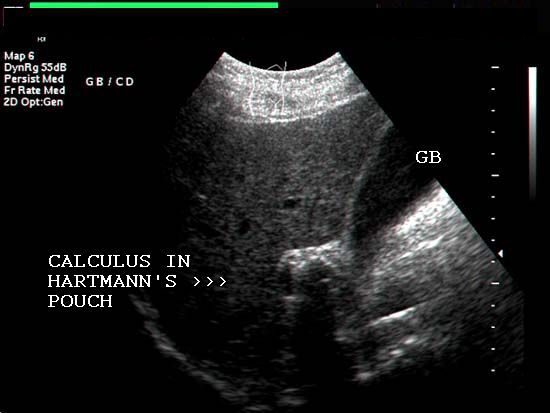

This case (another patient) showed a huge gall bladder with calculus lodged in the Hartmann's pouch. The gall bladder measured more than 4.8 cms. in width due to the obstructive nature of the stone. Ultrasound images are courtesy of Shlomo Gobi, Israel.
Reference: http://en.wikipedia.org/wiki/Gallstone
Limy bile

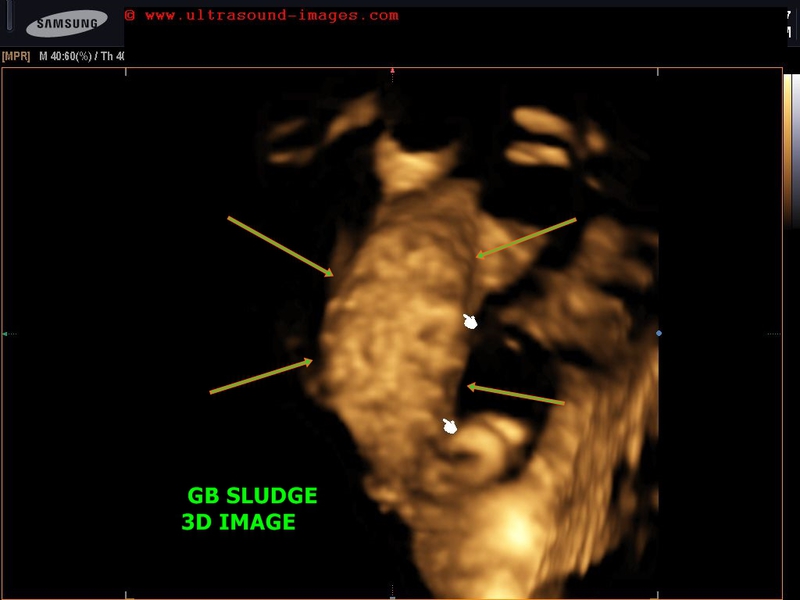
case-2: thick GB sludge causing hepatization of gallbladder- 3D ultrasound images
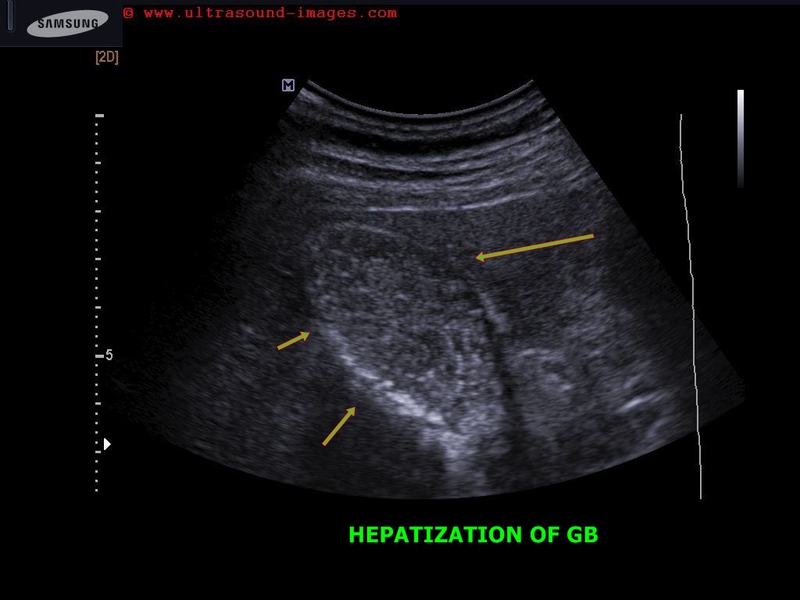
Synonyms: Biliary sand or lime bile or lime water bile in gall bladder
Sonography of the right hypochondrium shows a large distended gall bladder with markedly echogenic contents. The echogenicity appears similar to that of the liver (hepatization of the gall bladder). This ultrasound image suggests presence of limy bile in the gall bladder. This is caused by the collection of calcium rich salts within the organ and is an extreme form of biliary sludge. It is also known as Milk-of-calcium bile and is often associated with cholecystitis. Ultrasound image (upper most row- case-1) is courtesy of Prasenjeet Singh, MD, India. This image was taken using a Toshiba Nemio -30 system.
case-2: shows hepatization of gallbladder. Using a Samsung Accuvix ultrasound system.
Reference: http://www3.interscience.wiley.com/journal/112184176/abstract(free article)
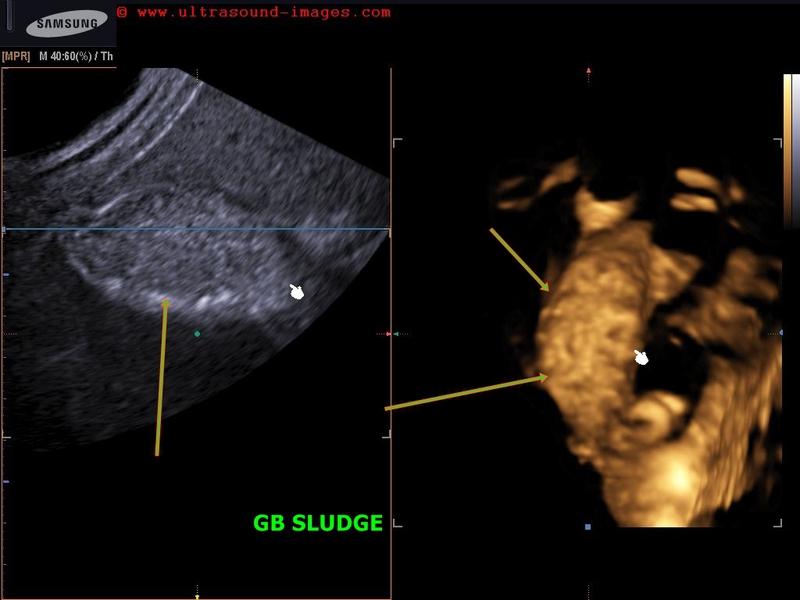
Gall bladder sludge

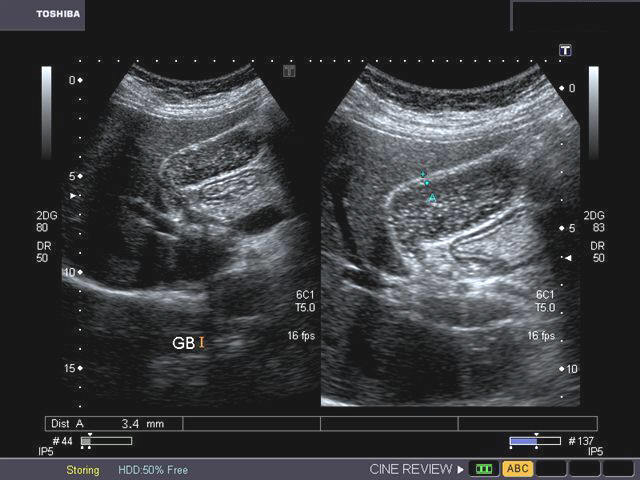
The presence of particulate matter, mainly calcium bilirubinate and cholesterol crystals forms biliary sludge. The above ultrasound images show thickened gall bladder wall (suggestive of cholecystitis) with the GB (gall bladder) lumen filled with echogenic debris which is typical of gall bladder sludge. Repeat sonographic examination usually reveals a normal anechoic gall bladder. GB sludge is usually associated with biliary stasis and /or cholecystitis. Ultrasound images are courtesy of Gunjan Puri, MD, India.
Tumefactive gall bladder sludge
This ultrasound image of the gall bladder shows echogenic, thick amorphous matter in the dependent part. This appearance is suggestive of tumefactive or thick biliary sludge in the gall bladder. This appearance can often be confused with gall bladder neopalsia. Color Doppler imaging would help show absence of vascularity within the sludge mass. Some acoustic shadowing is also present, posterior to the sludge in this image, indicating presence of minute GB calculi. Ultrasound image is courtesy of Vikas Shukla, MD, India.
Gall bladder sludge with layering
This ultrasound image shows typical layering of the biliary sludge within the gall bladder, collecting in its dependant part. This is seen on the right half of the image. The upper part of the gall bladder shows clear bile. The image on left half shows a small peri-cholecstic collection suggestive of inflammatory changes. Image courtesy of Dr. Vikas Shukla, MD, India.
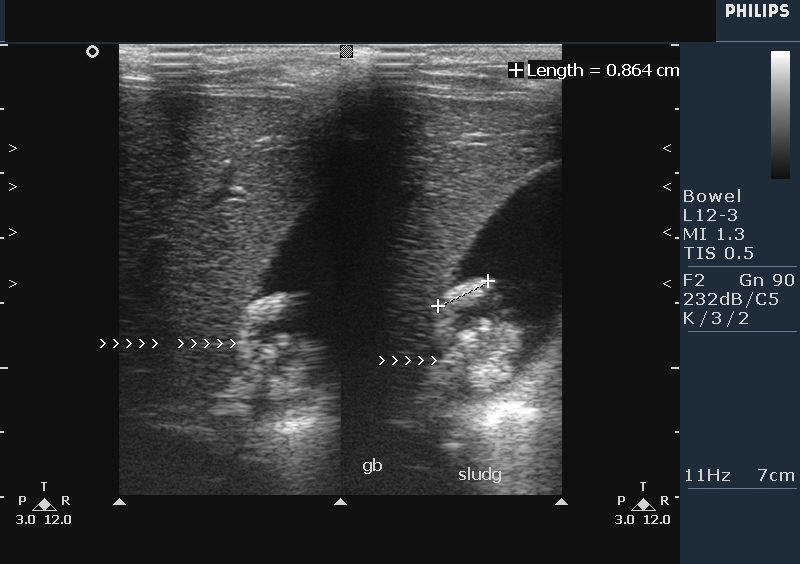
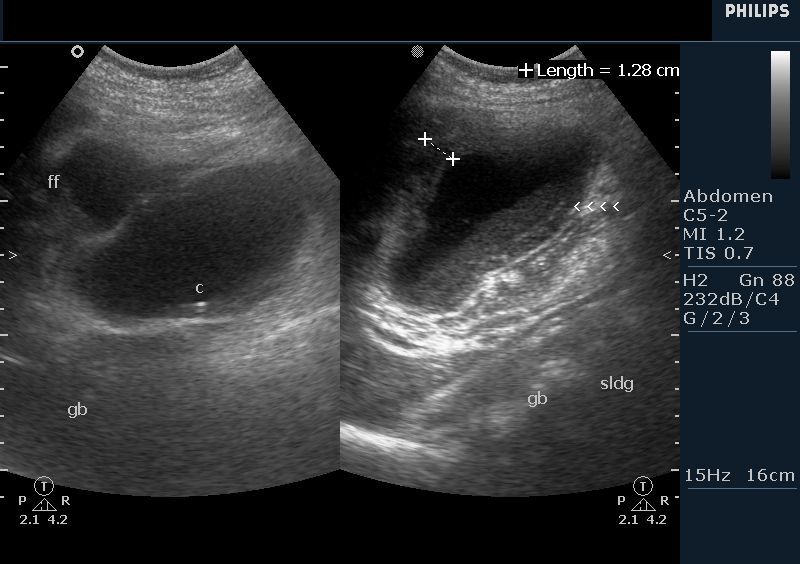
Gall bladder sludge simulating gall bladder neoplasm or mass


The above ultrasound images show an atypical sludge ball in the gall bladder. Note the variation in position and shape of what initially appeared to be a GB mass or neoplasm (possible malignancy). This kind of biliary sludge is semi solid. Color Doppler image (bottom) shows absence of flow within the "mass", clearly suggesting a biliary sludge ball as the final diagnosis. Images are courtesy of Dr. Dilraj Gandhi, MD, India.
Cholangiocarcinoma of CBD (common bile duct)
Dilated CBD with obstruction
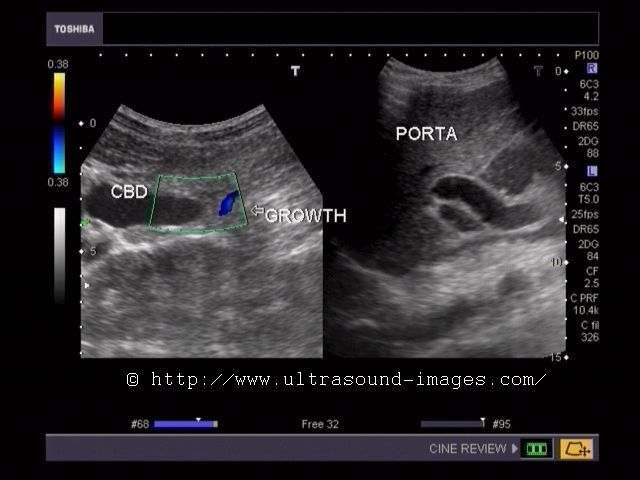
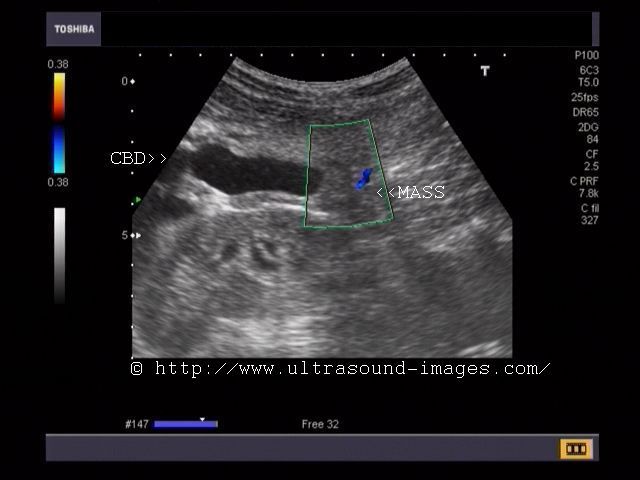
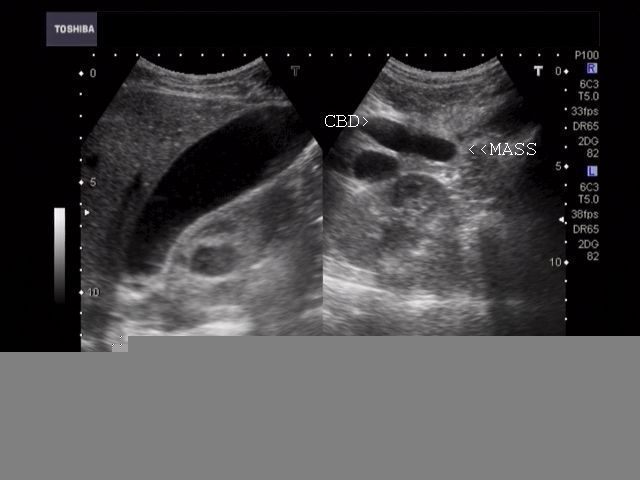

This patient had obstructive jaundice for which sonography of the liver and biliary tree was performed. Ultrasound images show a markedly dilated common bile duct (CBD) inside the porta hepatis with abrupt termination of the dilated CBD above the pancreas. Color doppler image of the common bile duct shows a vessel feeding the mass within the CBD. The liver showed marked dilation of the intrahepatic bilary tree (not shown here). These images suggest malignant mass of the supra-pancreatic part of the common bile duct, cholangiocarcinoma. There is also a right renal calculus (incidental finding). Depending on the morphology on sonography and radiological imaging, cholangiocarcinoma is classified into: exophytic- (tumor spreads outwards from the bile duct), infiltrative (tumor spreading along the walls of the bile duct), polypoid-(tumor shows polyp like mass within the bile duct or combined (a combination of one or more of the above mentioned types). In the case shown above, the ultrasound images suggest an exophytic variety of cholangiocarcinoma. Another classification based on the location of the tumors divides these into: intrahepatic and extrahepatic tumors. Intrahepatic cholangiocarcinoma is further classified into peripheral or hilar depending on the site of the tumor. Cholangiocarcinoma mass located at the junction of the right and left hepatic ducts is called a Klatskin tumor. These ultrasound images are courtesy of Dr. Vikas Arora, MD, India.
References:
http://radiographics.rsna.org/content/21/suppl_1/S97.full.pdf (free article and images)
http://radiographics.rsna.org/content/29/3/683.full.pdf+html(CT imaging of cholangiocarcinoma)
http://emedicine.medscape.com/article/365065-overview (free article on cholangiocarcinoma)
choledocholithiasis-CBD-calculus
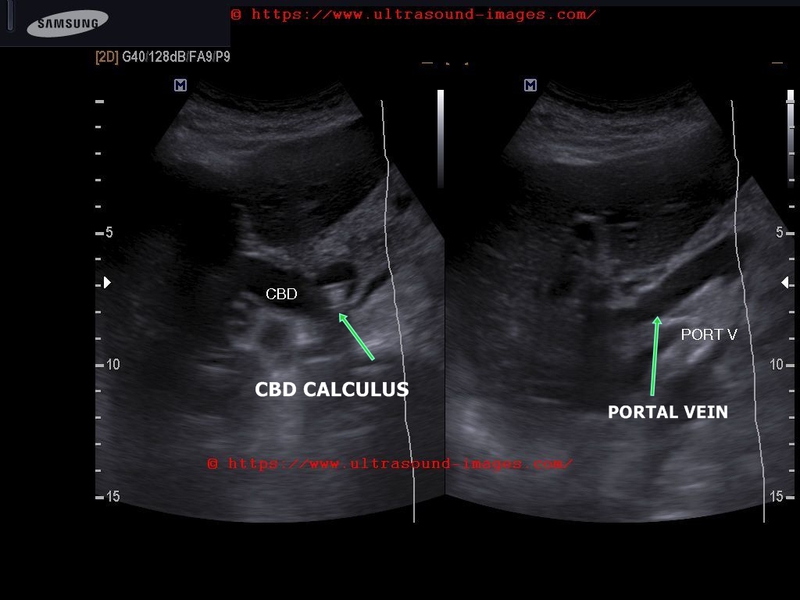

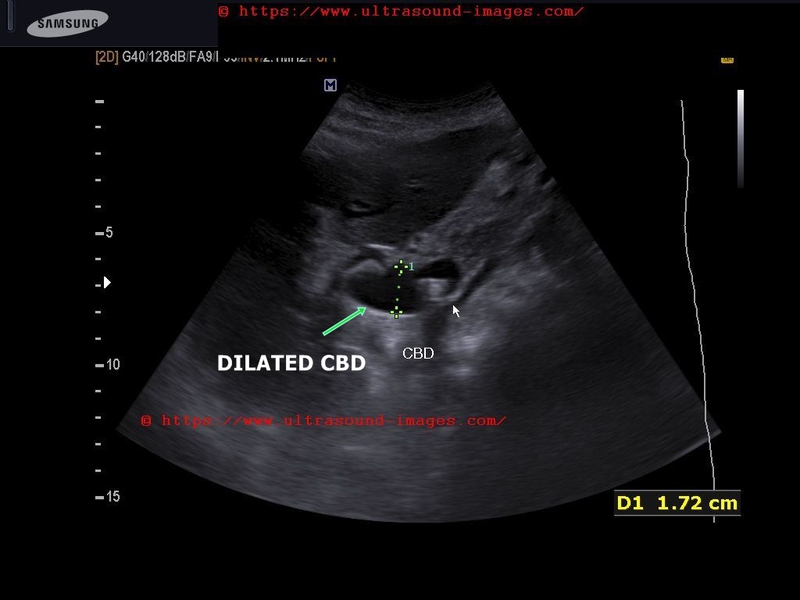
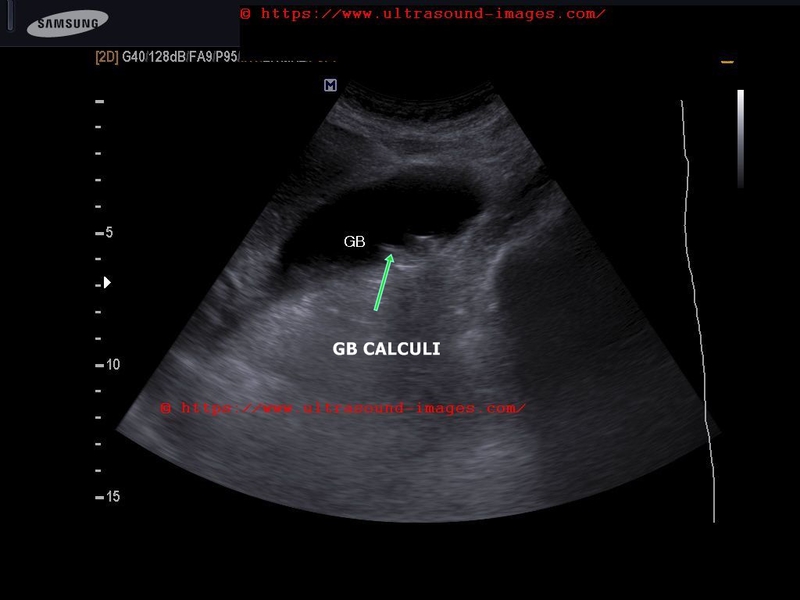

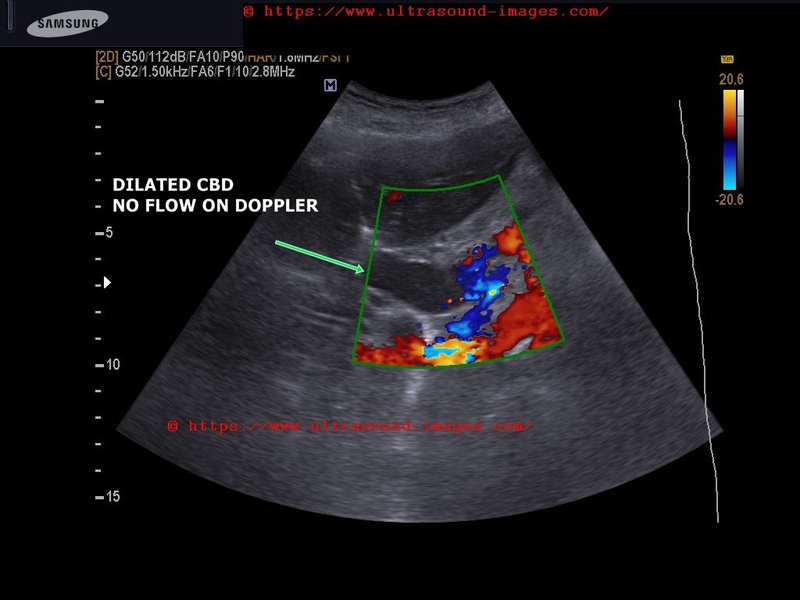
This elderly lady had obstructive jaundice due to CBD (common bile duct calculus) lodged in distal CBD. This condition is known as choledocholithiasis
= multiple GB (gallbladder) calculi present
= one of these calculi has lodged indistal CBD with resultant biliary obstruction
= resultant CBD dilatation is present with intrahepatic biliary tree dilatation also
(in this case the CBD measured 17 mm. (1.7 cms.)!!
= normal CBD diameter is < 6 mm (in post-chlecystectomy cases the width may be > 10 mm.)
= color Doppler is helpful in distinguishing CBD from portal vein (see the lower right image). CBD shows absence of color Doppler flow signal.
= in this patient CBD stent insertion resulted in reduction of bilirubin levels from 17 mg% to less than 7 mg%
References: Sonography of CBD calculus
© 2026, Joe Antony, MD All images and content in this site are copyrighted. www.ultrasound-images.com When visiting this site, we may use cookies to improve the performance of this site. Use of this site means you accept the use of cookies. Read our privacy policy at this page: https://www.ultrasound-images.com/privacy-policy/