
Ultrasound images of fetal chest
Contents of this page
- Pleural effusion in fetus
- Normal fetal Anatomy- Fetal aorta (aortic arch or arch of aorta and descending aorta)
- Case-2: Ductal arch compared to aortic arch- 34 weeks fetus
- Normal fetal anatomy: Fetal IVC (Inferior Vena Cava)
- Congenital diaphragmatic hernia- Left (CDH)
- Pulmonary sequestration in fetus
- Normal fetal thymus
- CHAOS-fetal-high-airway-obstruction-syndrome
- CCAM-congenital-cystic-adenomatoid-malformation
- Pulmonary-sequestration-extralobar-subdiaphragmatic
- Normal-fetal-esophagus
Pleural effusion in fetus
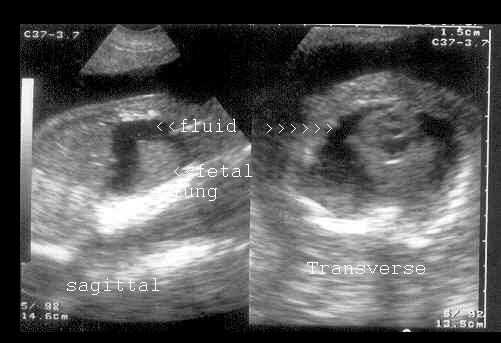


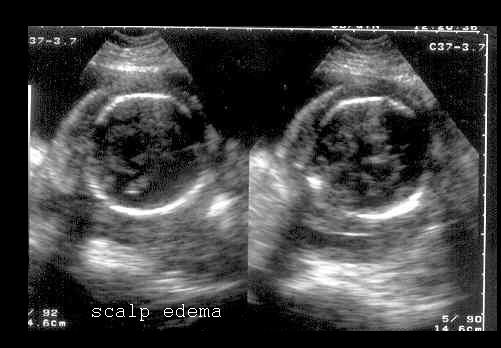
Fluid collection in fetal pleural cavity
This early third trimester pregnancy underwent routine sonography. Ultrasound images reveal large, bilateral pleural effusion in the fetus. Both the fetal lungs are virtually floating in the pleural fluid. There is also evidence of mild ascites and scalp edema in the fetus . Polyhydramnios is also present. These ultrasound findings suggest bilateral fetal pleural effusion with hydrops fetalis. Images courtesy of Dr. Prem Chand, Pakistan. These images were taken with a Toshiba Just Vision 200 ultrasound machine.
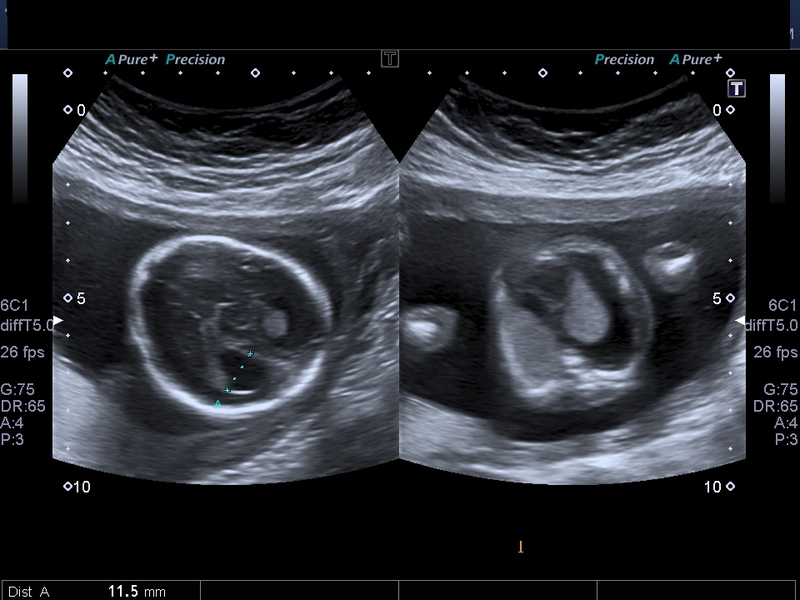
fetal hydrothorax- case-2
Download my E book for Amazon Kindle (download free Kindle reader for i Phone or Android)
Assorted ultrasound cases- by Joe Antony, MD
This is yet another example of Fetal hydrothorax, which is the term used for pleural effusion in the fetus. In this case there is a large pleural effusion or hydrothorax affecting the right lung. Unilateral hydrothorax usually involves the right side. This second trimester fetus shows the pleural effusion or hydrothorax completely encircling the fetal right lung. in this case the large right hydrothorax appears to have caused a complete collapse of the right lung. Such a large hydrothorax if present at birth can be life-threatening. The fluid usually contains chyle.
This ultrasound image is courtesy of Dr Durr-e-Sabih, FRCP.
Normal fetal Anatomy- Fetal aorta (aortic arch or arch of aorta and descending aorta)
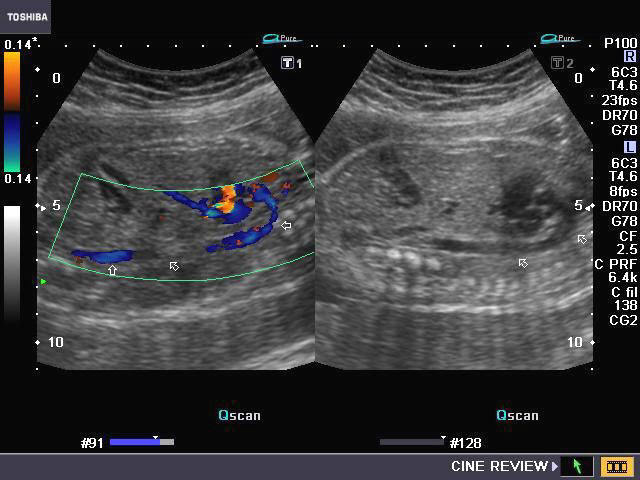
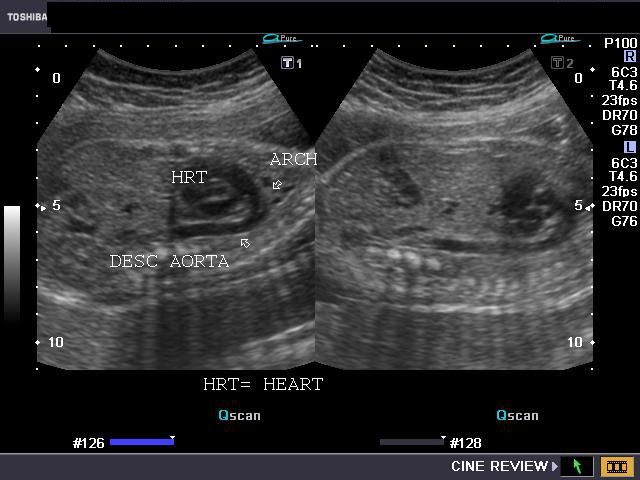
Fetal aortic arch Fetal ductal arch (left) and aortic arch (right)
These ultrasound and color Doppler images show a sagittal section of the fetal thorax with the aortic arch and the descending thoracic aorta seen emerging from the LVOT (left ventricular outflow tract).
The ultrasound image on right shows the sagittal section of the fetal ductal arch. The characteristic appearance of the fetal ductal arch is described as hockey stick whilst the aortic arch is compared to a candy stick or umbrella.
Ultrasound images taken by Joe Antony, MD, using a Toshiba Nemio-XG system.
Case-2: Ductal arch compared to aortic arch- 34 weeks fetus

This sagittal section image shows the fetal aortic arch. Note the typical shape of the ascending aorta and arch forming the candy stick shape as it descends downwards
Now compare the image above with the fetal ductal arch seen in the ultrasound images below



There is a clear hockey stick appearance to the fetal ductal arch as it has a shallow curve from the RVOT (right ventricular outflow tract) and descending downwards as the thoracic aorta. (see the red arrow). Images taken using a Philips HD 15 ultrasound system.
Normal fetal anatomy: Fetal IVC (Inferior Vena Cava)

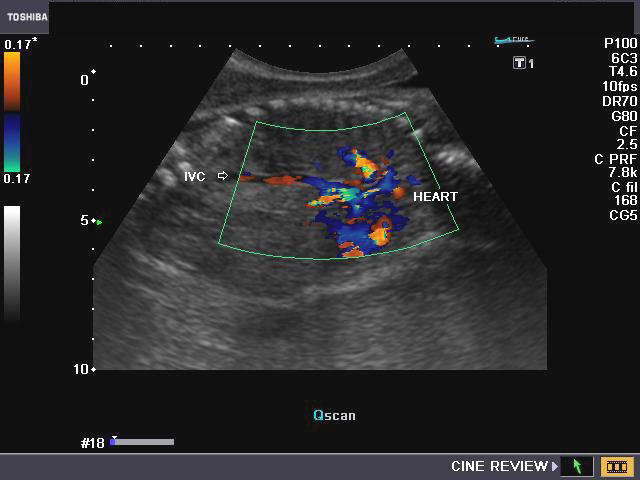
These ultrasound and Color Doppler images show the normal fetal IVC (Inferior Vena Cava) in sagittal section, entering the fetal right atrium after passing upward through the posterior aspect of the liver. One of the hepatic veins is also seen as it enters the IVC.
Congenital diaphragmatic hernia- Left (CDH)
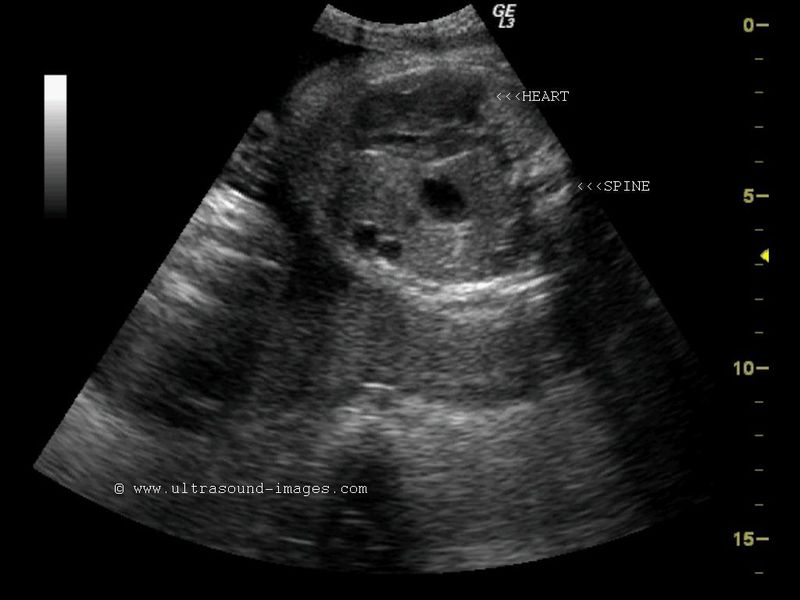

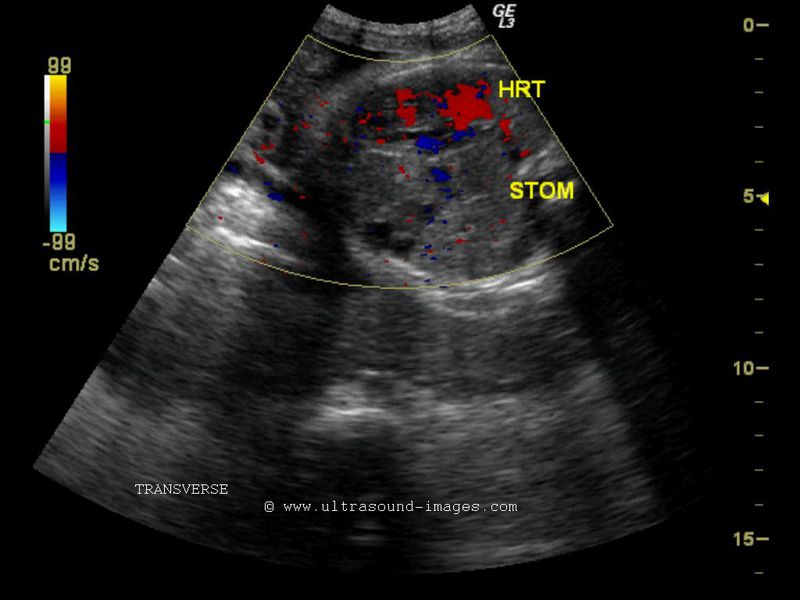
Transverse section fetal chest
CORONAL section fetal chest

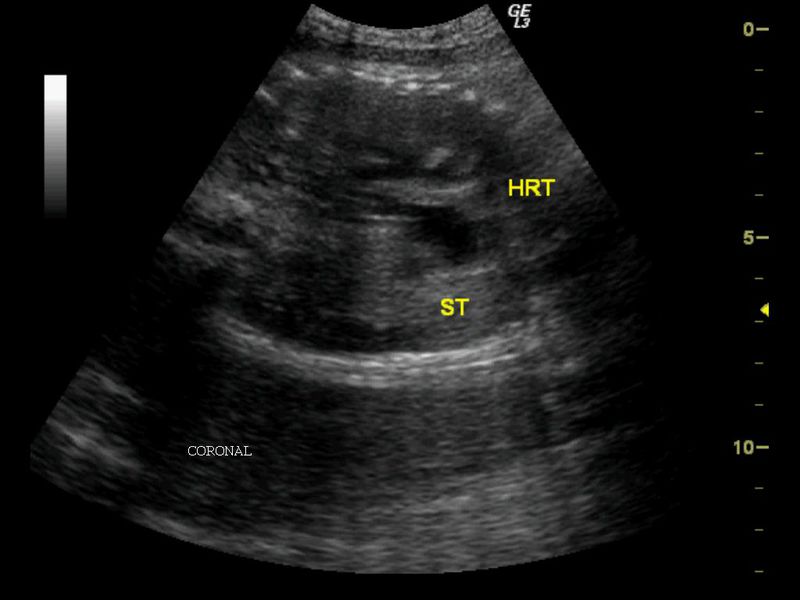
This was a 34 week old fetus with a remarkable congenital anomaly seen in the fetal chest. Transverse section ultrasound and color Doppler images show fetal stomach, left lobe of liver and fetal bowel in the left hemithorax. There is also evidence of midline shift of the mediastinal structures including heart to the extreme right of the fetal thorax. In addition, the fetal lungs appear markedly hypoplastic. (ST= stomach ; HRT= heart). The fetal left hemi- diaphragm is not visualized in these ultrasound images. These images are diagnostic of fetal CDH or left sided congenital diaphragmatic hernia. Left diaphagmatic hernia is far more common than hernia on right side. Early ultrasound imaging (2nd trimester) may fail to detect this fetal anomaly if the CDH is small or intermittent. This means that the herniated bowel and stomach may get replaced into their normal position at certain times and again enter the fetal chest at other times. This is a potentially lethal anomaly and may be associated with other fetal anomalies, the most common ones being cardiac defects. One of the diagnostic features of sonography of left CDH is the presence of stomach of the fetus in a transverse section of the fetal chest in the same view as a 4 chamber view of the heart.
References: http://www.fetalsono.com/teachfiles/CDH.lasso (free excellent article and images of CDH).
Pulmonary sequestration in fetus

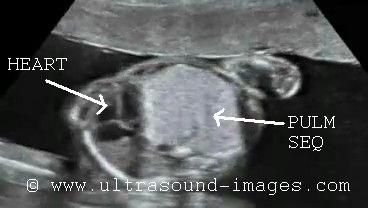

This late second trimester fetus shows a large, well defined mass lesion occupying the left hemithorax with displacement of the heart and mediastinal shift to the right side. Such an ultrasound appearance of an echogenic mass in the region of the left lung is typical of pulmonary sequestration. The main differential diagnosis here is congenital cystic adenomatoid malformation or CCAM as this is commonly known. Pulmonary sequestration may be intralobar (75 %) or extralobar (25%). The presence of a separate pleural cover around the sequestrated lung tissue is indicative of extra lobar pulmonary sequestration. If the pulmonary mass is located within the pleural cover of the lung it is called intralobar pulmonary sequestration. It is often difficult if not impossible to diagnose prenatally, intralobar sequestration. The presence of a feeder vessel usually arising from the thoracic aorta also goes in favour of the pulmonary lesions being extralobar pulmonary sequestration. Thus almost all pulmonary sequestration diagnosed during the fetal stage is extralobar in nature.
This case too, is extra lobar (supra-diaphragmatic) pulmonary sequestration. Likewise, intra-lobar pulmonary sequestration is a disease of adulthood.
Medical literature currently feels that an element of cystic changes with macro cysts may also be present in pulmonary sequestration thus leading to considerable overlap of cystic adenomatoid malformation and pulmonary sequestration.
These ultrasound images of pulmonary sequestration are courtesy of Dr Sunil Yadav, MD.
references:
1) http://www.ajronline.org/doi/full/10.2214/ajr.180.2.1800433
2) http://emedicine.medscape.com/article/412554-overview
Normal fetal thymus

The normal fetal thymus is seen well in this high resolution ultrasound image of the fetal chest (courtesy of Dr. Mayank Chowdhury, MD). The fetal thymus is shown highlighted within the dotted ring in this image. The normal fetal thymus is a hypoechoic homogenous tissue/ gland occupying the anterior mediastinum and is relatively large though variable in size. It is limited anteriorly by the sternum and posteriorly by the major cardiac vessels (seen here in 3 vessel view- namely the superior vena cava, ascending aorta and pulmonary artery). The ultrasound machine used here is the powerful Voluson E8 (GE) system.
References:http://www.fetalultrasound.com/online/text/3-195.HTM
CHAOS-fetal-high-airway-obstruction-syndrome




CHAOS-case-2-3D-ultrasound



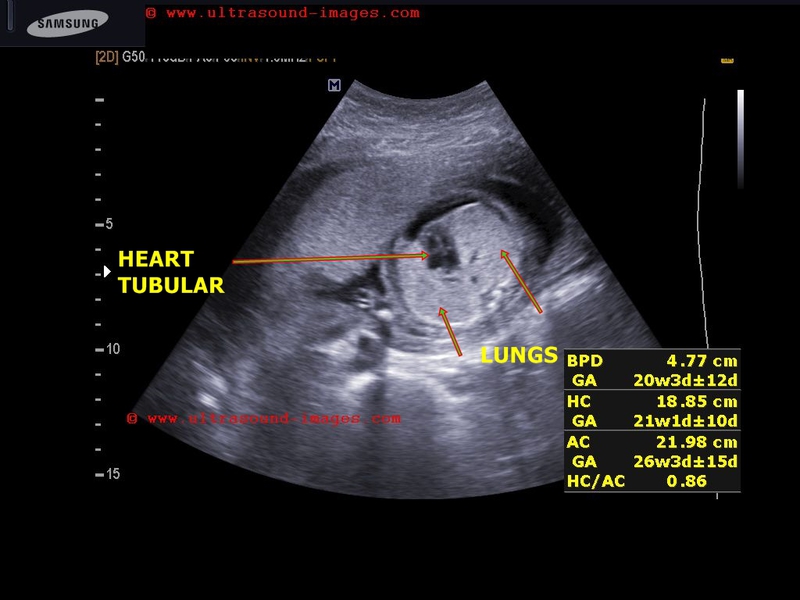

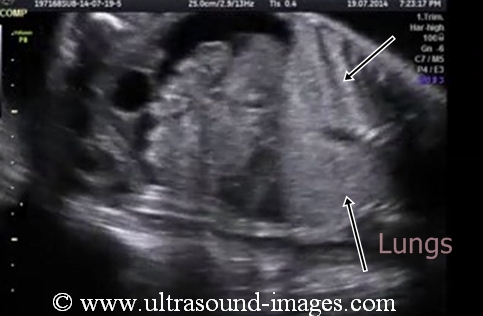
This early third trimester fetus shows certain characteristic ultrasound findings: (congenital high airway obstruction syndrome):
- markedly echogenic fetal lungs or hyperechoic lungs.
- inverted diaphragmatic convexity- the diaphragm is convex towards the fetal abdomen.
- the fetal trachea is markedly dilated and distended with fluid.
- evidence of fetal ascites.
- the fetal heart is markedly compressed by the enlarged and fluid distended fetal lungs resulting in a tubular compressed heart.
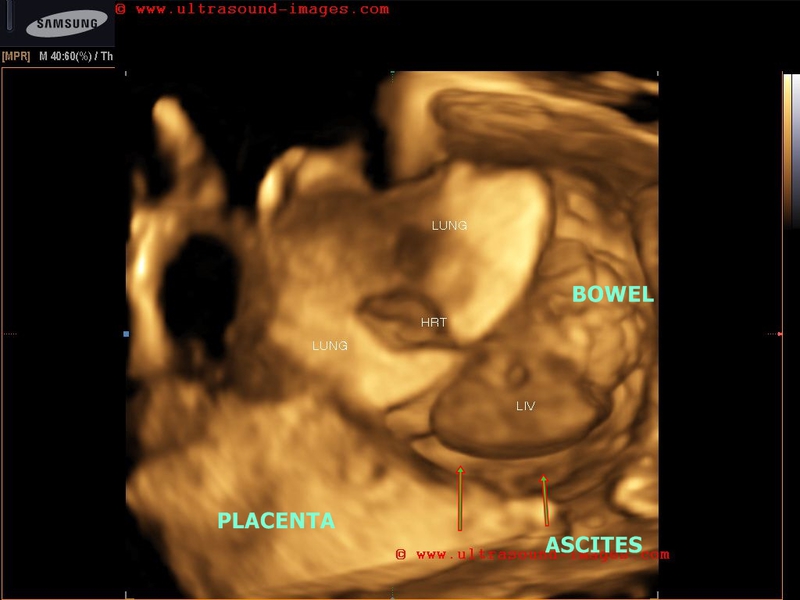
All these findings suggest obstruction at the level of the upper trachea or larynx (due to agenesis of larynx) resulting in fluid distension of the trachea and the lungs of the fetus. This causes the lungs of the fetus to be markedly enlarged compressing the fetal heart and pushing down the diaphragm resulting in a bell shaped diaphragm. All these ultrasound image findings point to only one possible diagnosis namely congenital high airway obstruction syndrome (CHAOS). These ultrasound images of congenital high airway obstruction syndrome are courtesy of Firoz Bhuvar, MD. The 3-D Ultrasound image also shows the typical features of congenital high airway obstruction syndrome (CHAOS) resulting in a distended belly and bell shaped abdomen and thorax.
Case-2:
3D ultrasound study of CHAOS in 20 weeks old fetus.
All the typical diagnostic features present.
CCAM-congenital-cystic-adenomatoid-malformation
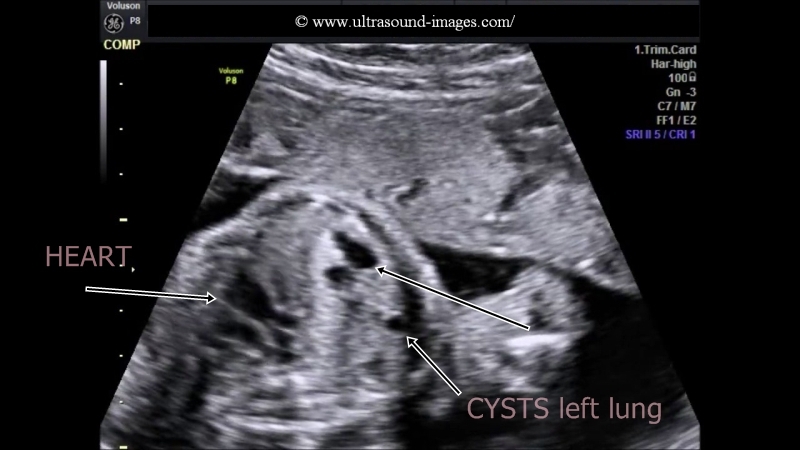
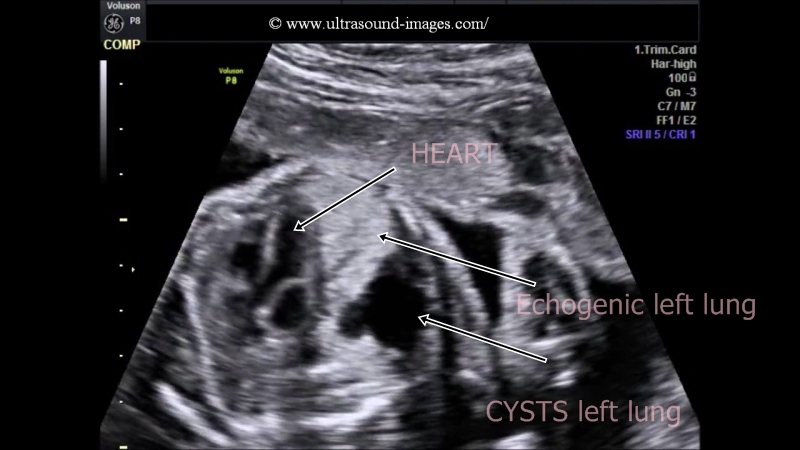

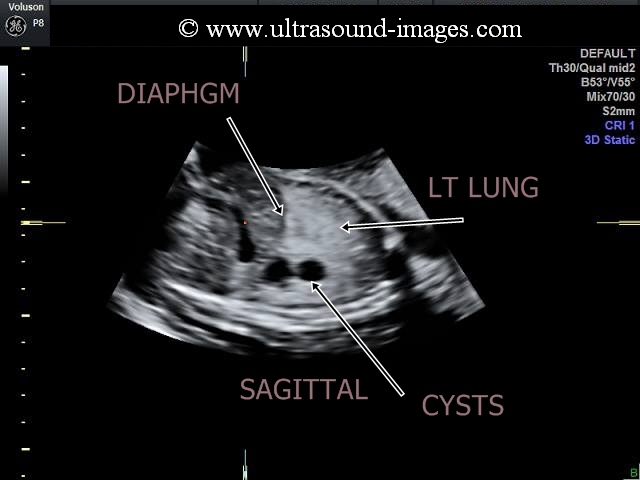


CCAM (Congenital cystic adenomatoid malformation) or CAML (cystic adenomatoid malformation of the lung) is a condition characterised by multiple cystic lesions within the mass in the Fetal lung which is part of a developmental anomaly resulting in disordered pulmonary parenchyma. there is a dilatation of the terminal respiratory bronchioles along with failure of formation of the normal alveoli of the Fetal lungs resulting in a mass which is similar to a hamartoma. The ultrasound findings have resulted in a grading of CCAM (Congenital cystic adenomatoid malformation) or CAML (cystic adenomatoid malformation of the lung) into three grades:
type I: CCAM with large cysts of 2 to 10 cms.
type II: CCAM with small cysts of sizes 0.5 to 2 cm
type III: CCAM which is solid or micro cystic
the case described here is of the type I or macro cystic with very large cysts in the left lung of the fetus. congenital cystic adenomaotid malformation or CCAM also known as cystic adenomatoid malformation of the lung is also associated with marked echogenicity and enlargement of the affected part ( usually only one lobe of the lung). CCAM almost invariably involves one lobe and is usually unilateral. In this case, the left lobe is severely involved with enlargement of the affected lung, multiple and large cysts formation. The fetal heart is displaced to the right side. All these ultrasound image findings are suggestive of congenital cystic adenomatoid malformation of the lung. These 2D and 3-D ultrasound images of CCAM are courtesy of Firoz Bhuvar, MD.
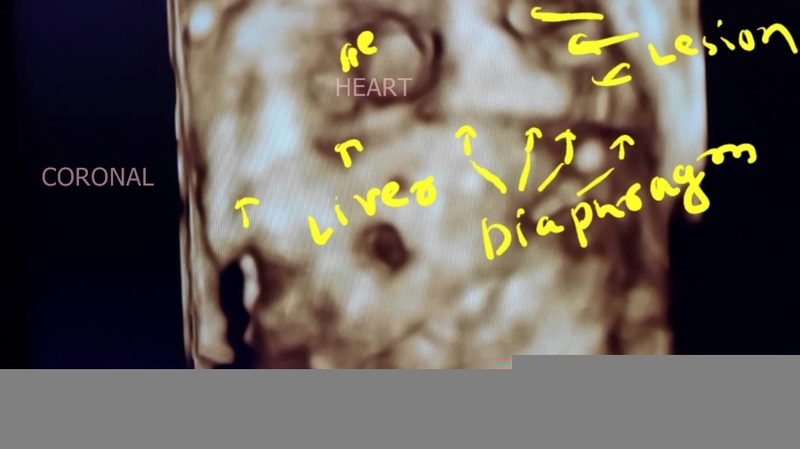
Pulmonary-sequestration-extralobar-subdiaphragmatic

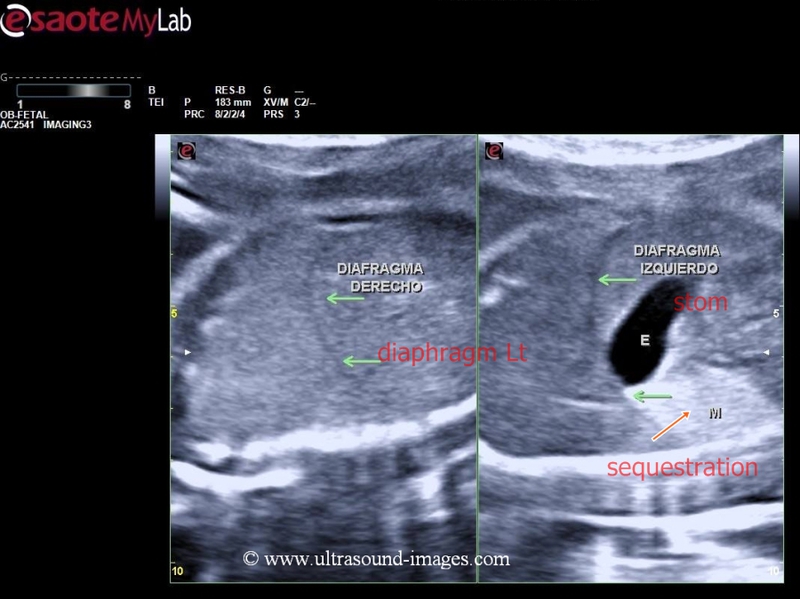
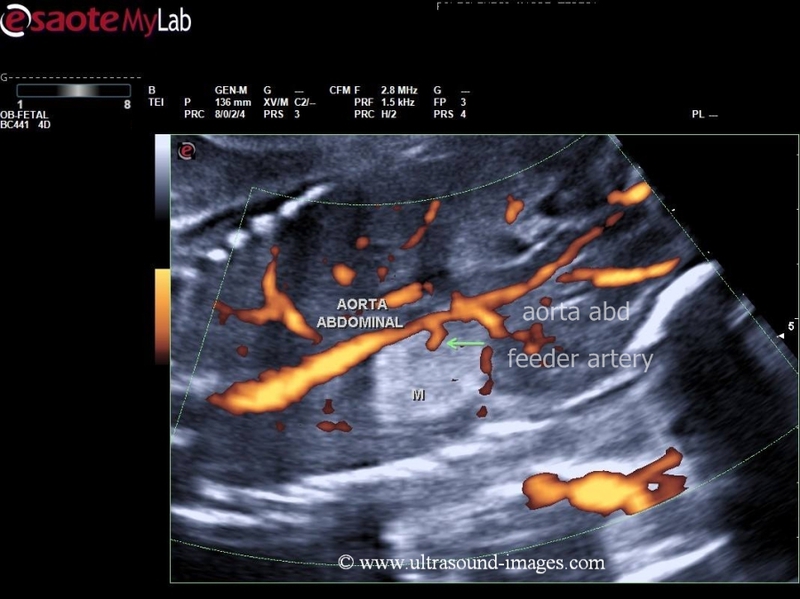
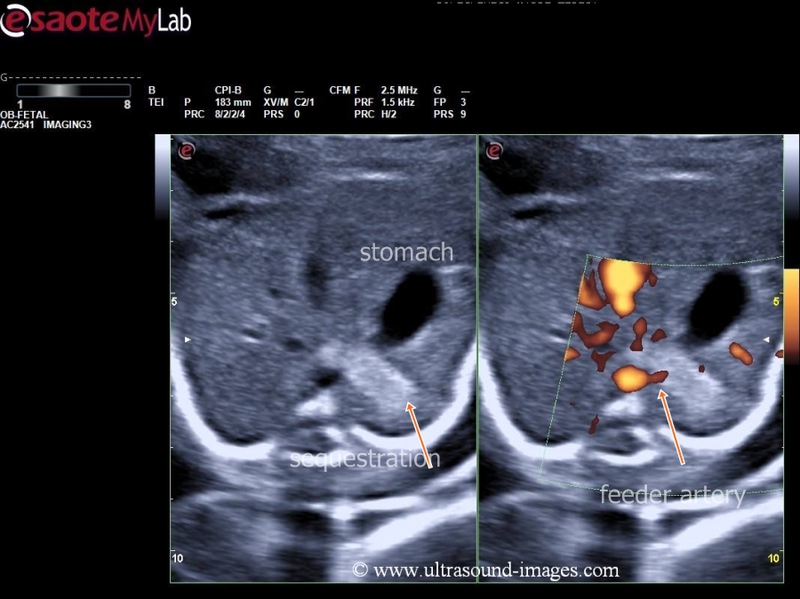
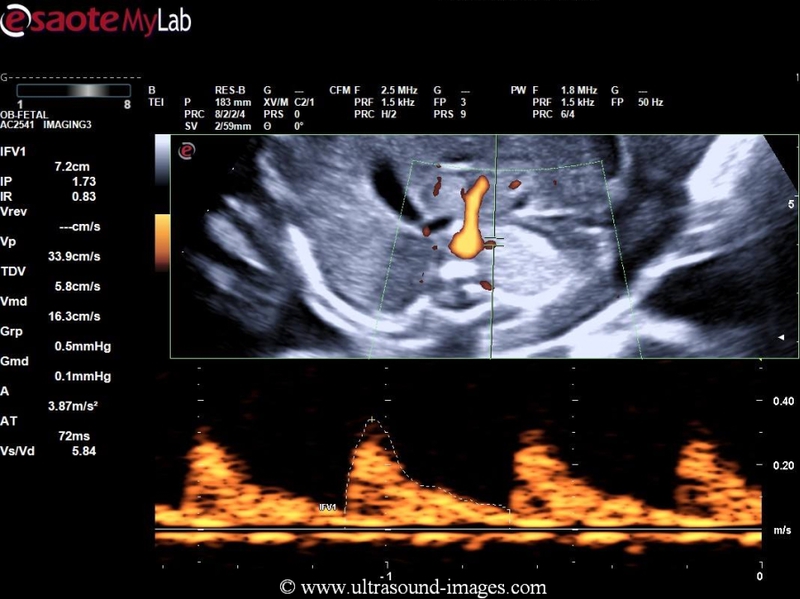
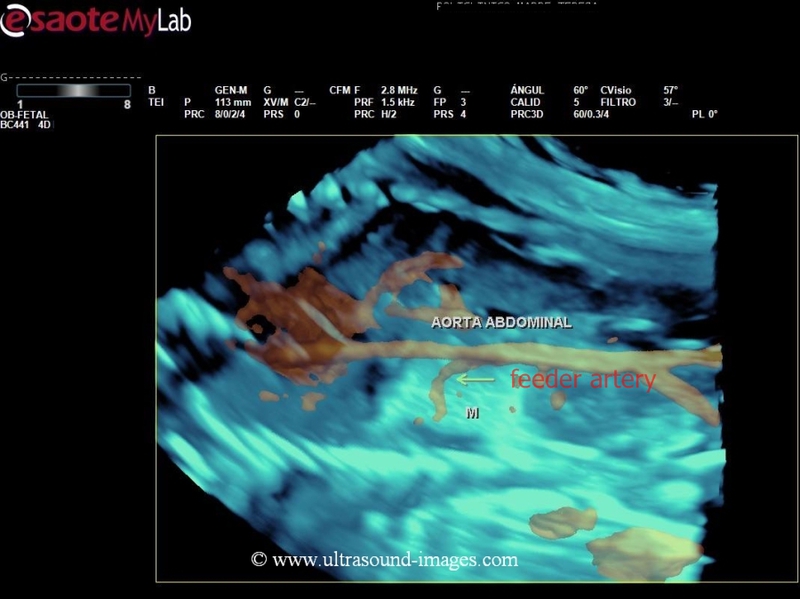
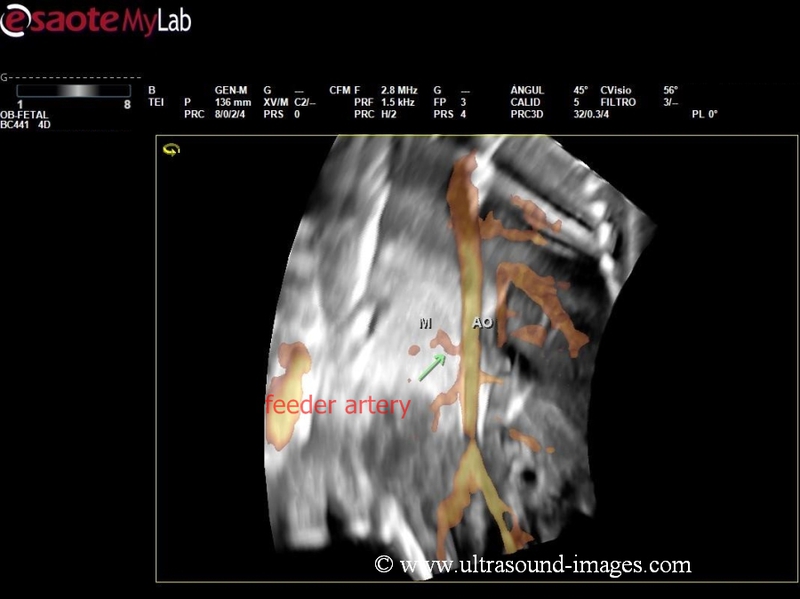
The 2D, 3D and colour Doppler ultrasound images above show a case of extralobar, sub-diaphragmatic left-sided pulmonary sequestration. 2-D ultrasound shows an echogenic mass of 3 x 2.7 cm located below the left dome of diaphragm and adjacent to the fetal stomach. 3-D ultrasound and 4D color Doppler ultrasound show a feeder vessel which is an artery originating from the abdominal aorta supplying this echogenic mass. The echogenic mass in question is the sequestrated lung located below the left dome of the diaphragm. These ultrasound and 3-D colour Doppler images are courtesy of Jorge Hernandez, MD.
As stated in an earlier case, on this page, pulmonary sequestration is characterised by an echogenic area of lung which does not drain nor is connected to the bronchial tree. The sequestration also has its own blood supply separate from that of the rest of the lung. Almost all of the cases of pulmonary sequestration diagnosed prenatally are extralobar in nature. Pulmonary sequestration is classified into two subtypes- intralobar and extralobar. Extralobar pulmonary sequestration is further classified into supradiaphragmatic and infradiaphragmatic subtypes.
Normal-fetal-esophagus
The ultrasound images above show normal fetal esophagus in the axial plane seen fully distended (arrows)and collapsing completely (3rd image) as the peristaltic wave passes downwards. The esophagus is seen anterior and slightly to the right of the thoracic aorta and behind the left fetal atrium. In the axial plane the fetal esophagus is seen as a ring shaped cystic structure when fully distended with ingested amniotic fluid. Lack of filling or failure to empty may signify fetal esophageal anomalies such as esophageal atresia or tracheo-esophageal fistula. The sonologist must also inspect the fetal stomach bubble and its normal presence is proof of a normal upper gastro-intestinal tract. These images and the ultrasound video below are courtesy of Firoz Bhuvar, MD.
© 2026, Joe Antony, MD All images and content in this site are copyrighted. www.ultrasound-images.com When visiting this site, we may use cookies to improve the performance of this site. Use of this site means you accept the use of cookies. Read our privacy policy at this page: https://www.ultrasound-images.com/privacy-policy/