
Pancreas
Contents of this page
- Ultrasound images of normal pancreas
- Ultrasound images showing age related fatty change of the pancreas
- Calcification/ calculi in pancreas
- Pseudocyst of the pancreas
- Case-2: Pancreatic pseudocyst
- Carcinoma of pancreas
- Carcinoma of pancreas- case-2
- Dilatation of MPD (main pancreatic duct)- complication of acute pancreatitis
- Dilated main pancreatic duct due to calculus
- acute-pancreatitis-sonography
Ultrasound images of normal pancreas
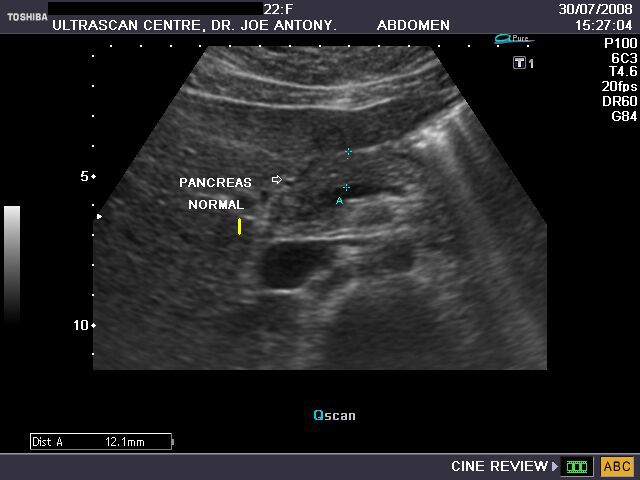
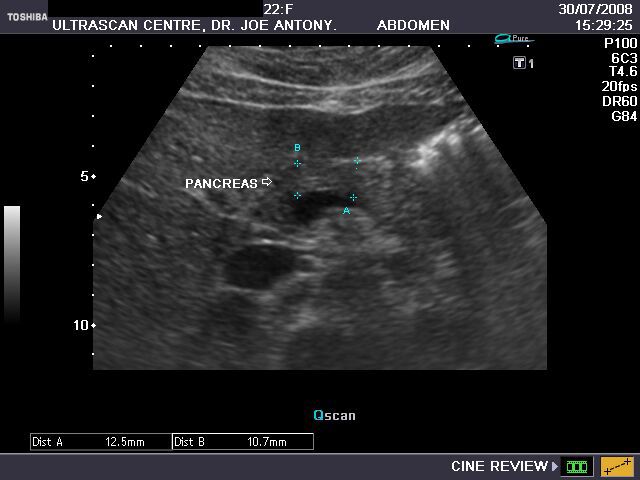
Transverse section of pancreas.
These ultrasound images show the normal pancreas in a young adult. It is seen as a thin strip of tissue, of about the same echogenicity (isoechoic) as the liver, and measures 10 to 14 mm. in thickness at the neck and body. The pancreas has both an endocrine (it secretes the insulin and glucagon hormones) as well as an exocrine function (it secretes a number of digestive enzymes). The pancreas in collaboration with the thyroid gland is intricately involved in the processing of glucose. Obesity often plays havoc with the functioning of both thyroid and insulin production by the pancreas and may result in the development of diabetes.
Ultrasound images showing age related fatty change of the pancreas
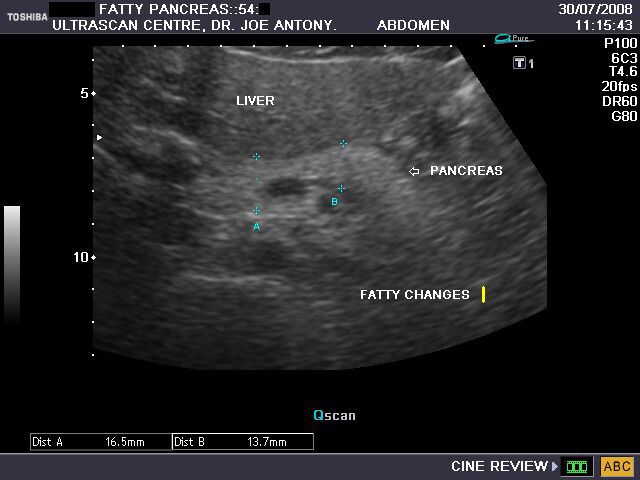


The above sonographic images of the pancreas in a middle aged patient show marked increase in the echogenicity of the pancreas, making it hyperechoic to the liver. This is the result of a combination of age related fatty change within this organ. There is also evidence of fatty change of the liver.
Calcification/ calculi in pancreas




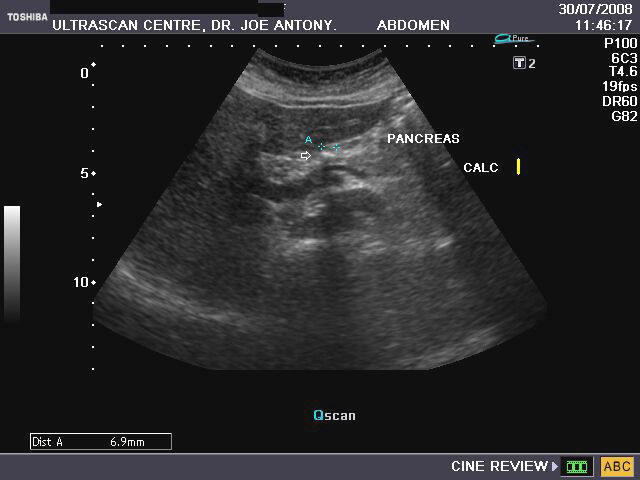
The above images show both calcification or calculi in the pancreatic body (4 to 7 mm. size) and also hyperechoic pancreatic tissue. This patient is an elderly female with epigastric pain. All ultrasound images by Dr. Joe Antony, MD, India. Machine used here is the Toshiba Nemio XG.
Pseudocyst of the pancreas


This patient presented with abdominal pain. Ultrasound images reveal a large cystic collection with thickened and shaggy walls, located anterior to left kidney and in close relation to tail and body of the pancreas. These ultrasound findings suggest a diagnosis of pseudocyst of the pancreas. The pancreas may show calcific lesions (not visualized here) in such cases. Images courtesy of Dr. Gunjan Puri, Surat, India.
Reference:
1) http://www.emedicine.com/med/topic2674.htm(free article)
Case-2: Pancreatic pseudocyst
Transverse section of pancreas
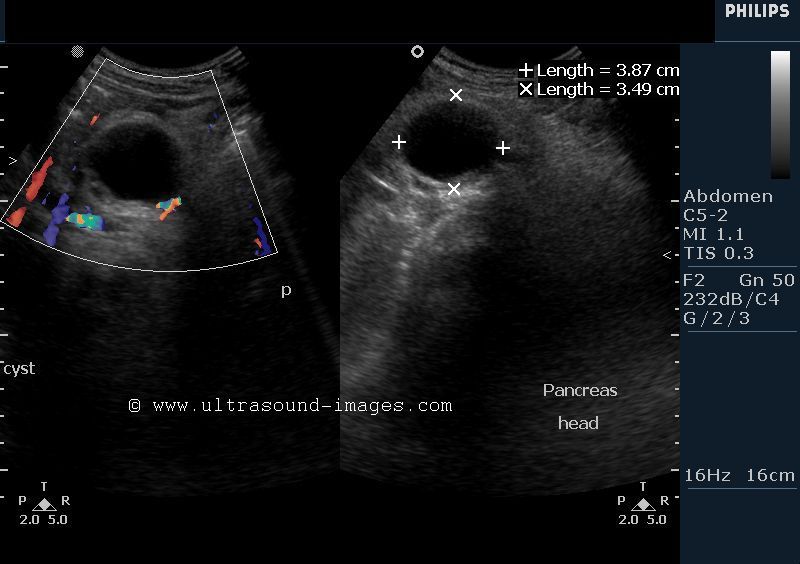

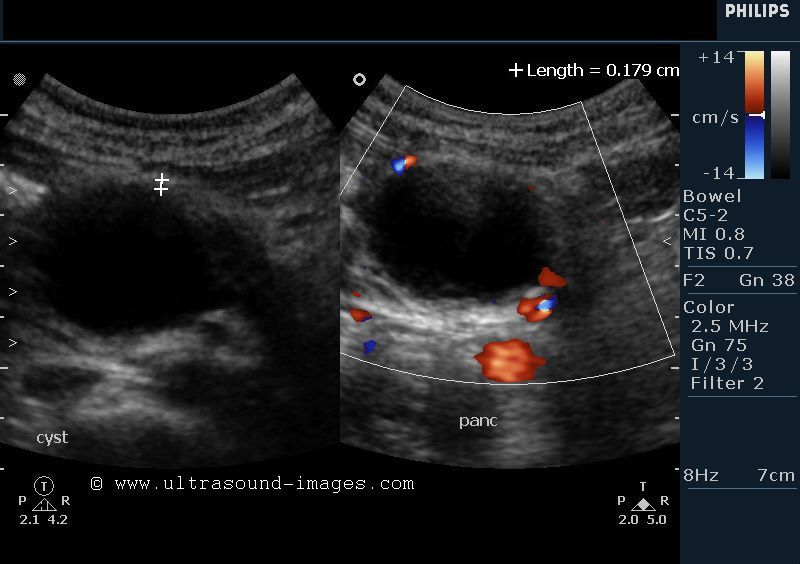
This was a young adult female patient. Sonography shows a cystic mass (3.5 x 3.9 cms.) having shaggy, thick walls in relation to the head of the pancreas. Some particulate debris is present in the dependent part of the cystic mass, but septae are absent. Color Doppler images of the cyst reveal absence of color flow within the cyst ruling out a vascular mass. These ultrasound imaging findings favor a diagnosis of pseudocyst of the pancreas. Pseudocysts are the commonest cause of cystic lesions of the pancreas and are formed as a result of extravasation of pancreatic enzymes into the surrounding spaces. These pancreatic enzymes produce strong inflammatory exudative response from the adjacent peritoneal membranes with fluid sealed within a collagenous wall (of the cyst). These ultrasound images are courtesy of Dr. Vikas Shukla, MD, India.
Carcinoma of pancreas



This elderly female patient presented with obstructive jaundice . Sonography showed intrahepatic biliary duct dilatation with markedly dilated CBD (common bile duct) with a 2 cms. sized hypoechoic mass in the head of the pancreas. Abrupt termination of the CBD at the level of the pancreatic head mass was noted, suggesting that this mass was the cause of the dilated CBD. The main pancreatic duct appeared normal. These ultrasound imaging findings are typical of a pancreatic carcinoma. The main differential diagnoses in such cases are chronic or acute pancreatitis. Ultrasound images of pancreatic carcinoma are courtesy of Dr. Prasenjeet Sngh, MD, India
References:
http://emedicine.medscape.com/article/280605-overview
http://www.radiologyassistant.nl/en/43848b63def9d
Carcinoma of pancreas- case-2
Color Doppler image of portal vein and CBD

Color Doppler image- dilated intrahepatic biliary tree
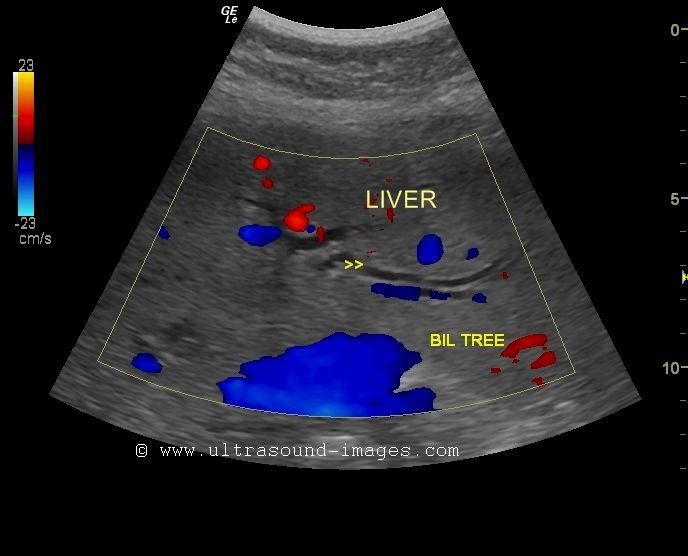

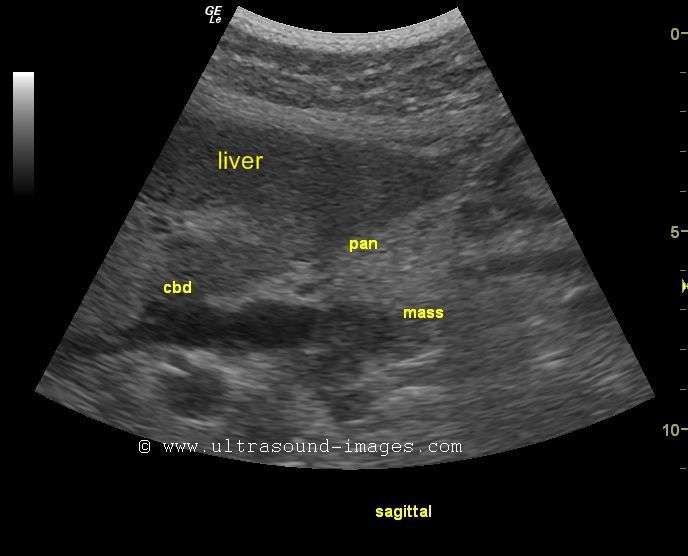
This was again an elderly female patient who presented with obstructive jaundice of unknown etiology. Sonographic imaging of the liver shows dilated intrahepatic biliary tree with a dilated Common bile duct (13 to 14 mm. in diameter). The color Doppler study of the intrahepatic part of the biliary tree shows the absence of color Doppler signals (absence of color) in the biliary tree as opposed to the color signals in the hepatic and portal vein branches. This is also seen in the common bile duct which also shows no color as opposed to the portal vein which shows intense color. This enables easy identification of the biliary tree from the blood vessels. The reason is because of the sluggish flow of bile in the biliary ducts (with no color signals) as compared to the rapid blood flow within the portal and hepatic veins (producing intense color signals). Ultrasound image of the pancreas shows a hypoechoic mass of 15 mm. in the head of the pancreas with the CBD abruptly terminating at this level. These ultrasound and color Doppler images suggest carcinoma (cancer) of the head of the pancreas with common bile duct obstruction. The commonest malignancy of the pancreas is adenocarcinoma of the pancreatic ducts (90 % of pancreatic cancers). This patient will be further investigated by endoscopic ultrasonography and CT scan imaging. The liver in this patient did not show evidence of metastases.
References: http://emedicine.medscape.com/article/370909-overview
Dilatation of MPD (main pancreatic duct)- complication of acute pancreatitis


Transverse section image of dilated MPD:
This adult patient had a history of acute pancreatitis some time ago. On following up this case, sonography of the pancreas showed a markedly dilated main pancreatic duct (MPD) measuring 15 mm. in width. One of the sequelae of acute/ chronic pancreatitis is fibrosis of part or whole of the pancreas, and resultant obstruction to the pancreatic duct. In the images above, the obstruction to the main pancreatic duct has occurred at the head of pancreas. Such changes in the pancreas are also present in chronic obstructive pancreatitis. Ultrasound images are courtesy of Dr. Prasenjeet Singh, MD, India.
References:
Article on pancreatitis- Cleveland clinic
http://radiographics.rsna.org/content/29/4/1003.full (free article and images)
http://emedicine.medscape.com/article/371772-overview
Dilated main pancreatic duct due to calculus


Ultrasound image- dilated pancreatic duct: Calculus in pancreatic duct:
This middle aged lady had h/o dyspepsia for which sonography of the pancreas was done. Ultrasound images show markedly dilated main pancreatic duct (5 mm.) with a calculus (stone) seen as an echogenic nidus in the terminal part of the main pancreatic duct, within the head of pancreas. Pancreatic duct calculi are seen within the main pancreatic duct whilst echogenic foci in the pancreatic gland itself are called calcifications. Both pancreatic calcification and calculi are usually the result of chronic pancreatitis and are more common in alcoholics. Ultrasound images of pancreatic duct calculus are courtesy of Dr. Prasenjeet Singh, MD, India.
References:
Article on sonography of chronic pancreatitis
http://www.joplink.net/prev/200509/02.html
http://www.hbpdint.com/upload/PDF/20108410446172943.pdf
acute-pancreatitis-sonography
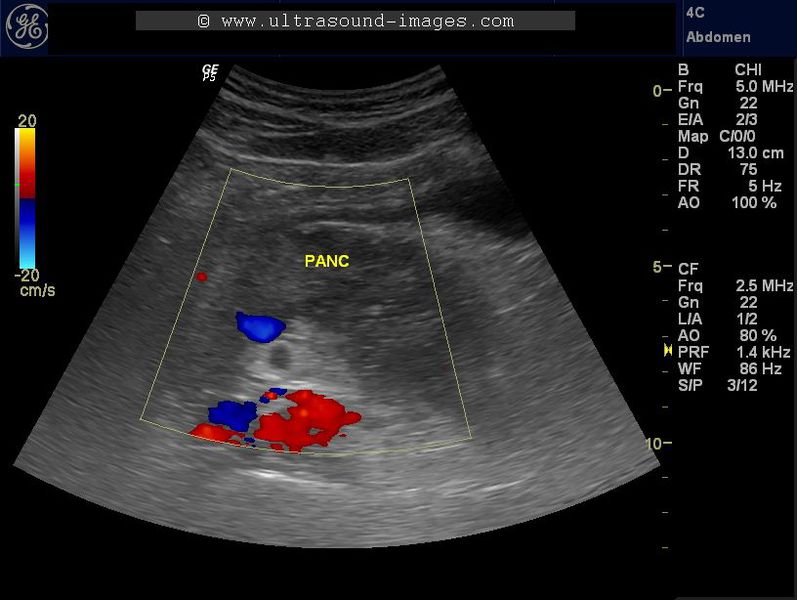

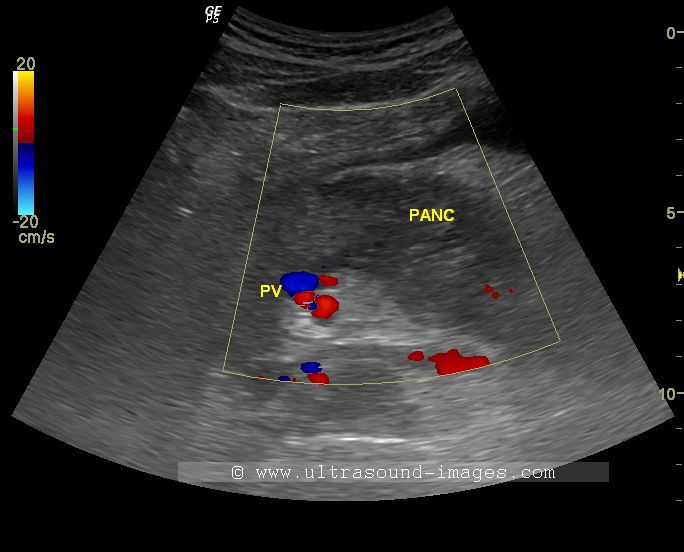
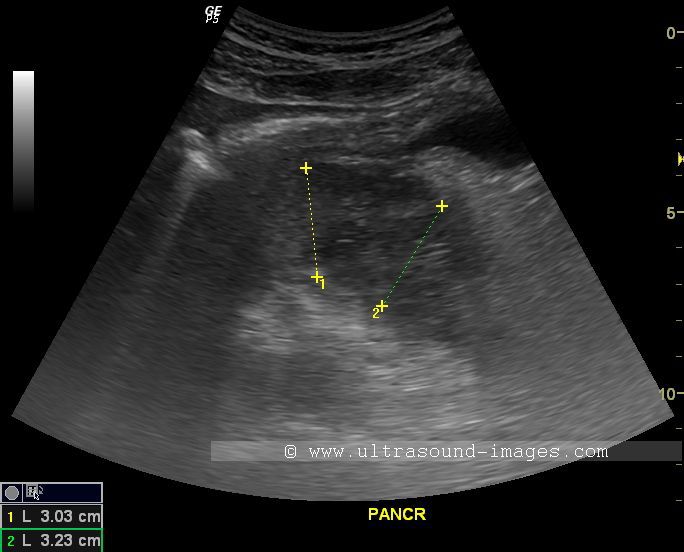

Pancreatitis is defined as inflammation of the pancreas. Pancreatitis may be acute or chronic. Acute pancreatitis is characterised by sudden inflammation of the pancreas and may be mild or severe.
Mild pancreatitis is sonographically visualised as a swollen oedematous pancreas with inhomogenous echotexture and poorly defined margins of the pancreas. There may be fluid around the margins of the pancreas and in certain cases pseudocyst may also be present in close relation to the pancreas.
Severe pancreatitis is usually associated with focal or widespread necrosis of the pancreas.in severe acute pancreatitis, there may be widespread organ dysfunction and treatment would have to be prompt to prevent severe morbidity or even in certain cases, mortality. Mild acute pancreatitis can be treated conservatively and has excellent prognosis.
The ultrasound images above reveal a case of acute pancreatitis following alcohol intake in a known alcoholic. The images show swollen, oedematous pancreas with inhomogeneous echotexture as described above. The anteroposterior diameter of the pancreas varies between 2.5 to 3.5 cm in this case, with a global increase in the volume. There is also evidence of minmal peri-pancreatic fluid in this patient. Colour Doppler ultrasound also was done, but which showed little or no vascularity of the pancreas in this patient. Ultrasound image of the pelvis shows a small amount of fluid around the sides of the urinary bladder, also evidence of the inflammatory process of the pancreas.
References:
© 2026, Joe Antony, MD All images and content in this site are copyrighted. www.ultrasound-images.com When visiting this site, we may use cookies to improve the performance of this site. Use of this site means you accept the use of cookies. Read our privacy policy at this page: https://www.ultrasound-images.com/privacy-policy/