
Uterus
Contents of this page
- Dystrophic calcification of uterus
- Calcified fibroid
- Ultrasound image of Pedunculated fibroid
- Fibroid in pregnancy
- Types of fibroid
- Pyometra
- Infections of the uterus
- Migrated IUCD
- Congenital anomalies of uterus
- Hypoplastic uterus
- Foreign body in cervix of uterus
- Uterine arterio-venous malformations
- Adenomyosis of uterus
- Case-2: Adenomyosis
- Case-3: Adenomyosis
- Asherman's syndrome: Uterine synechiae
- Pedunculated polyp of the cervix
- Pedunculated fibroid of the cervix
- Case-2: Pedunculated fibroid of cervix
- Nabothian cysts of the cervix
- Lipoleiomyoma of uterus
- Cystic hyperplasia of endometrium
- Endometriosis of urinary bladder
- Carcinoma of the cervix
- Endometrial hyperplasia
- 3D-ultrasound images normal uterus
- 3D-ultrasound images septate uterus
- subseptate uterus with pregnancy
- septate uterus- 3D images case-2
- multiple polyps of the endometrium
- 3-D ultrasound images of endometrial polyp
- 3-D ultrasound bicornuate uterus with non communicating horn
- hydrosalpinx-fallopian-tube
- 3D-ultrasound-copper-T-IUCD
- congenital-anomaly-rudimentary-horn-of-uterus
- endometrial-cast-cervix
- unicornuate-uterus-3D-ultrasound
- Endometrial-junctional-zone-contractions
- retained-products-ultrasound-video
- cervical-hydrops-stenosis
- Hydrosalpinx
Dystrophic calcification of uterus

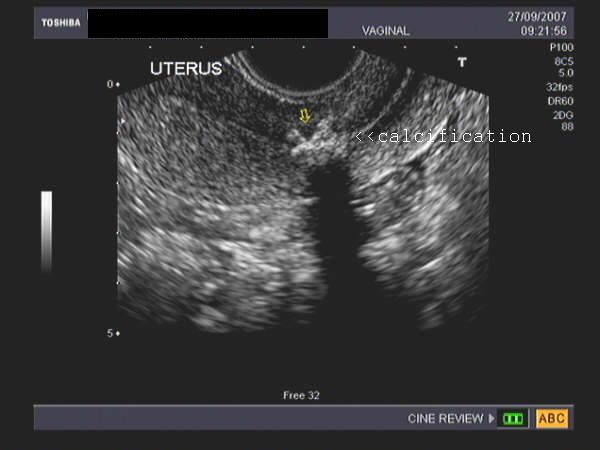
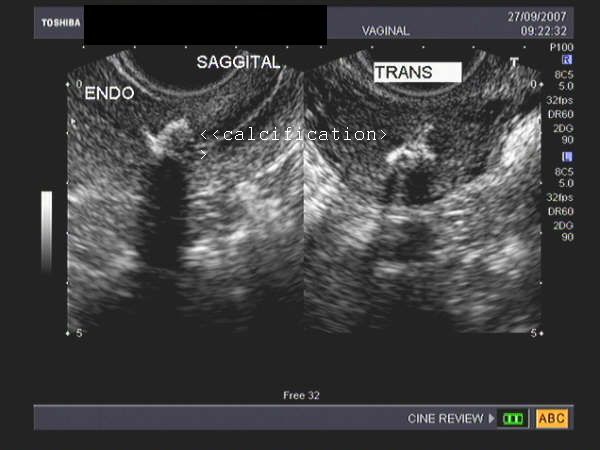


These sonographic images of the uterus reveal a dense calcification involving the inner myometrium and endometrium. This 23 yr. old female had a history of curettage. The diagnosis- dystrophic calcification of the uterus. The cause is usually instrumentation or procedures like curettage. These have little clinical significance. However, bony remnants of any previously aborted fetus must be excluded (see reference below). Images courtesy of Dr. Jaydeep Gandhi, Mumbai, India.
Reference:
http://www3.interscience.wiley.com/cgi-bin/abstract/104555335/ABSTRACT (abstract)
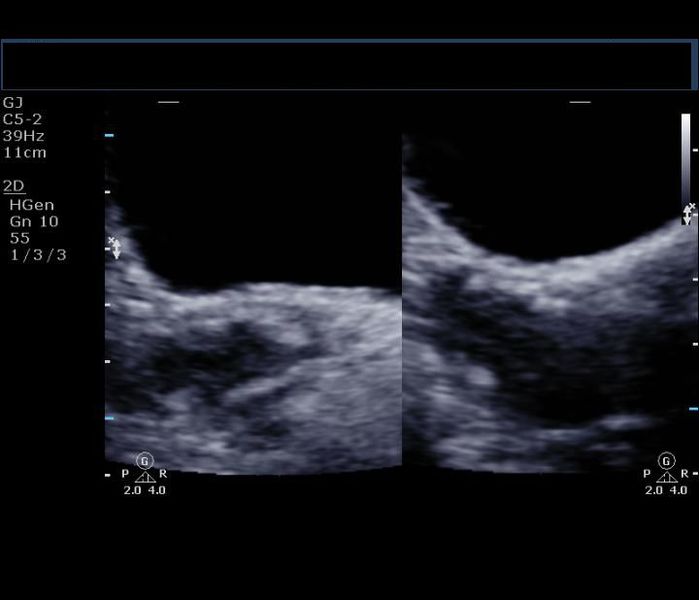
Calcified fibroid
Sonography of fibroid with calcification
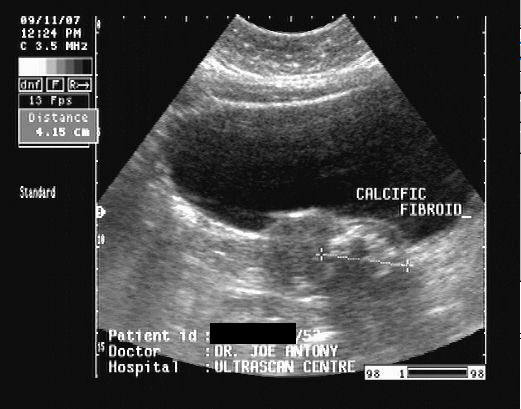
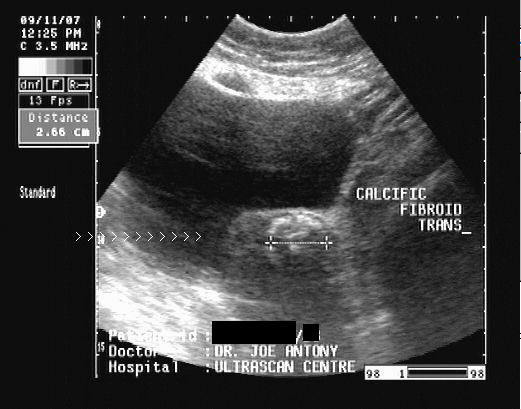
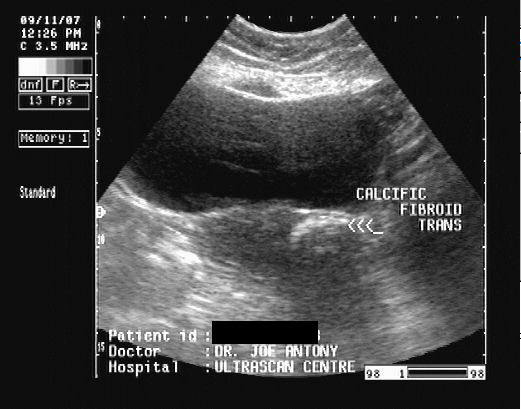
This middle aged female patient complained of pain in the suprapubic region. Ultrasound imaging revealed a small uterus with a calcific well-defined, intramural mass in the lower part of the body of uterus. There is clear acoustic shadowing posterior to the calcific lesion. These findings suggest a calcific fibroid of the uterus. Fibroids are often known to undergo calcificaiton in elderly females.
Reference: http://www.emedicine.com/radio/topic777.htm (free article)
Case-2: Calcification in fibroid: (C- shaped calcific fibroid)
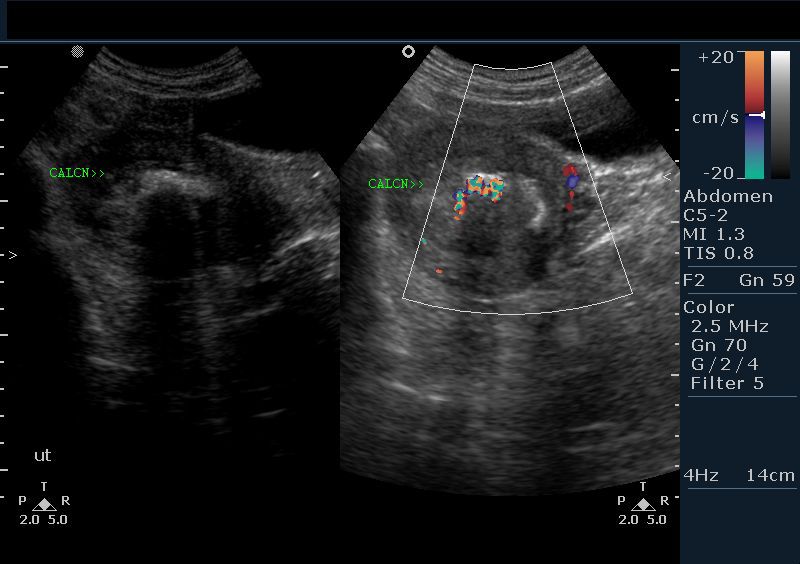
This intramural fibroid shows abundant calcification along the rim in a C-shape. Color Doppler image shows no significant vascular abnormality, except for some degree of "twinkling artefacts". Calcification of fibroids may occur as a peripheral ring or as popcorn type. Ultrasound image above is courtesy of Dr. Vikas Shukla, MD, India.
Case-3: Ring calcification of uterine fibroid


Fibroids can also show a complete ring of calcification, as in the ultrasound images shown in case-3 above. The fibroid shows a dense peripheral calcific rim, within the intramural mass that occupies the fundus and body of the uterus. The ultrasound image on the right is a 3D rendering of the calcific ring in the fibroid. The striking resemblance to a fetal head is amazing. Images are courtesy of Dr. Ravi Kadasne, MD, UAE.
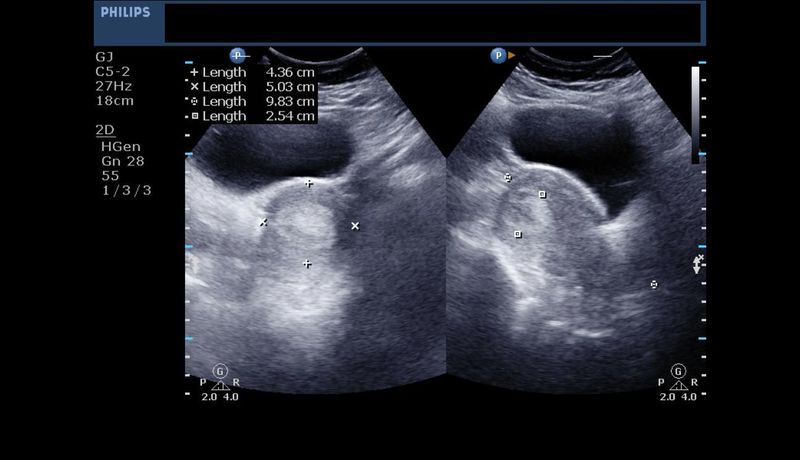
Ultrasound image of Pedunculated fibroid
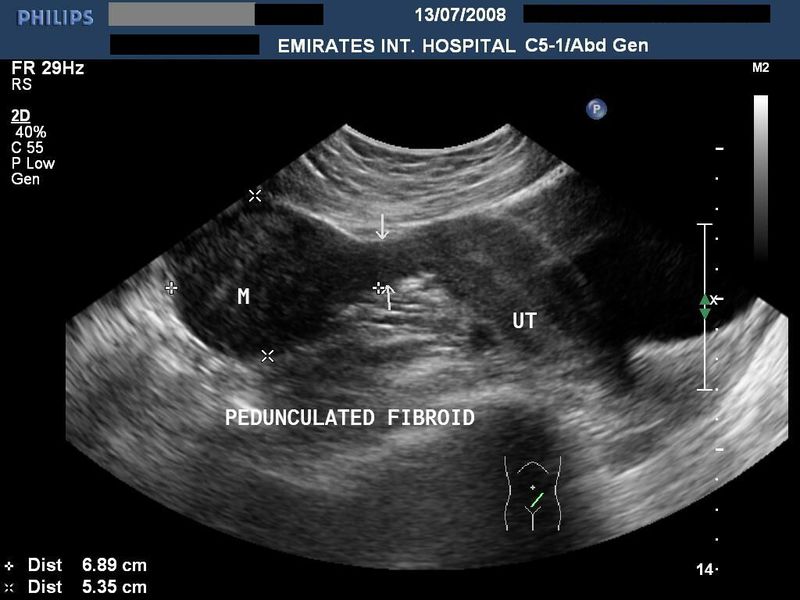


case-1 (image top left): Sonography of the uterus was done in this patient. Ultrasound image reveals a moderately large fibroid (7 x 5.3 cms.) connected to the fundus of the uterus by a thin stalk (peduncle). Ultrasound image courtesy of Dr. Ravi Kadasne, UAE. Machine used here is the Philips iu 22.
case-2: images on top left: also show a pedunculated fibroid. This 40 yr old lady presented with a mobile firm mass in the mid abdomen!!
These 2 images of pedunculated fibroid captured on a Samsung Acuvix- XG sonography machine.
Fibroid in pregnancy
Case-1: Fibroid in body of uterus

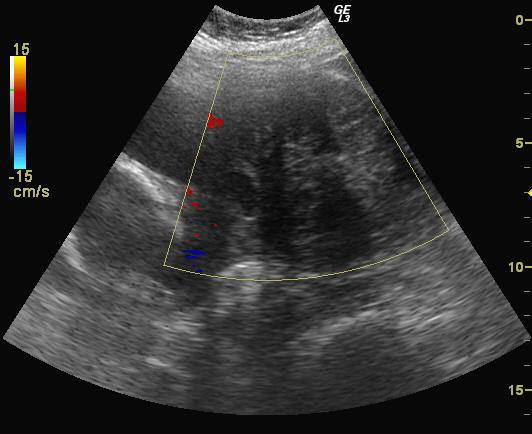
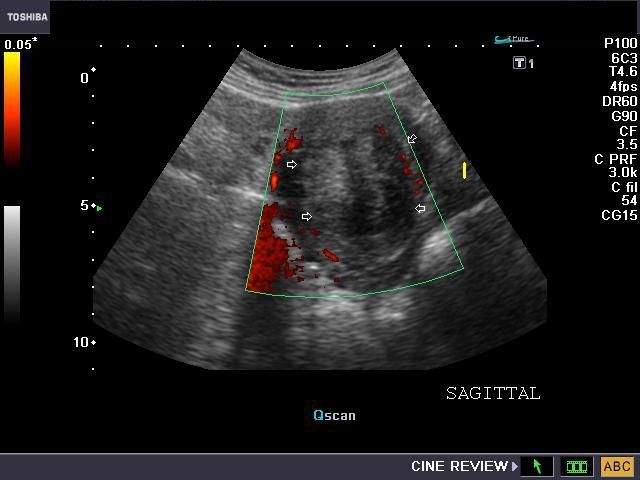
These ultrasound and color Doppler images show a gravid uterus (with 3rd trimester fetus), and a solid, inhomogenous, poorly vascular mass in the anterior wall of the uterus, bulging into the uterine cavity. Note the hypoechoic areas within the mass suggesting possible degenerative changes. These images are diagnostic of a pregnancy with fibroid. Ultrasound images courtesy of Dr. Ravi Kadasne, UAE; he used the Philips iu 22 machine for these stunning pictures.
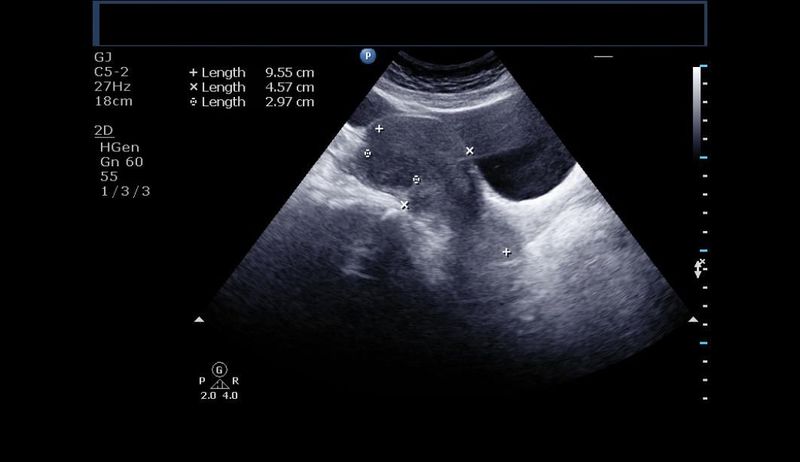
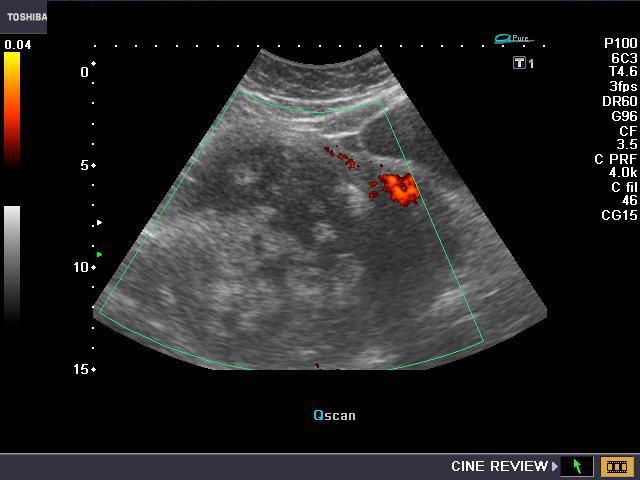
Case-2: Early pregnancy with fundic fibroid of uterus

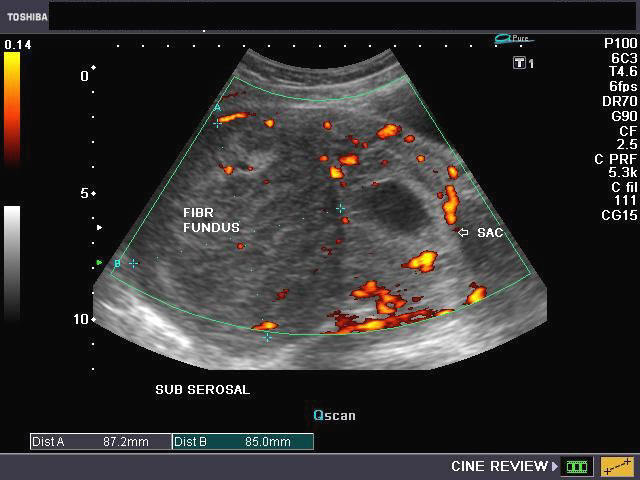
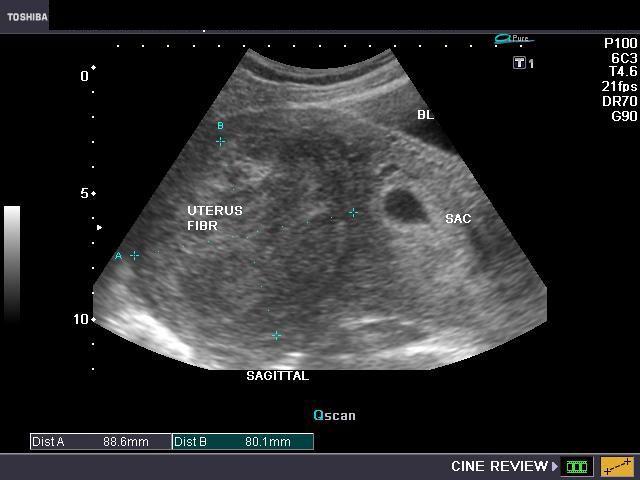
The 3 ultrasound pictures above show an early gestation sac (with a viable embryo), and a large fibroid in the fundus of the uterus. The mass (FIBR= fibroid), shows absence of degenerative changes or calcification despite its large size (almost 8 x 9 cms.). Power Doppler image of the uterus (image on top right) shows rim of vessels around the fibroid. Such early pregnancies with large fibroids have a high risk of abortions.
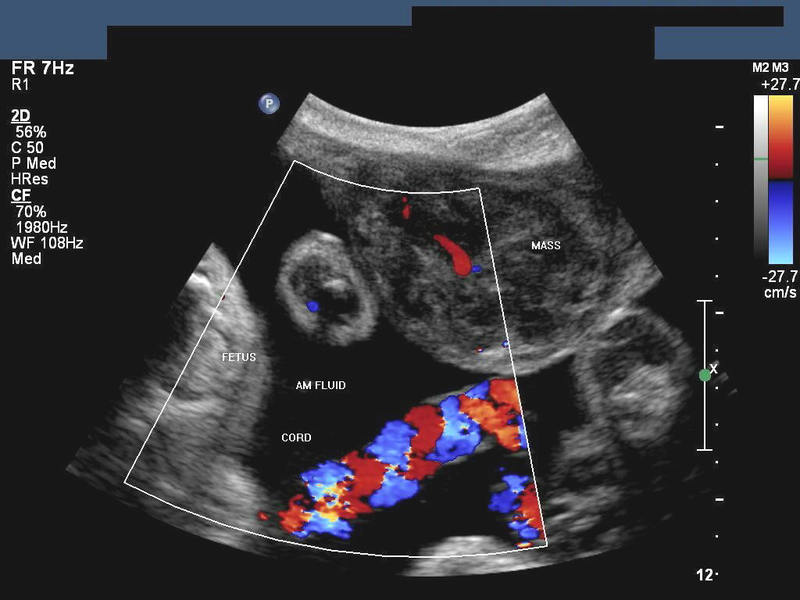
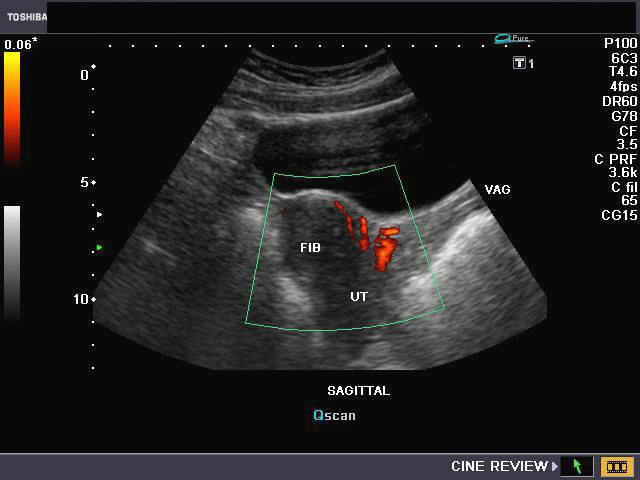
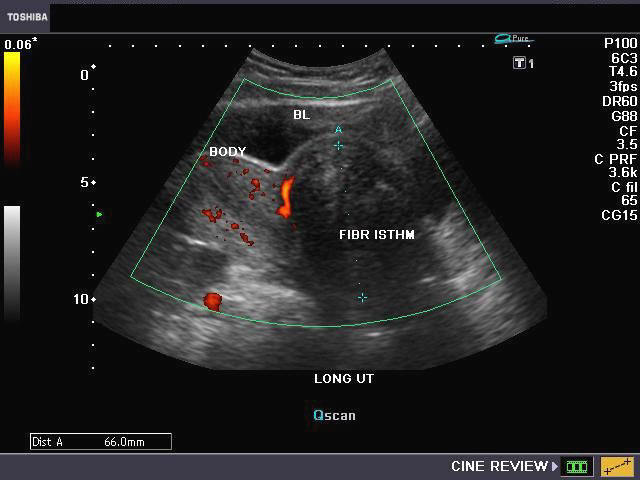
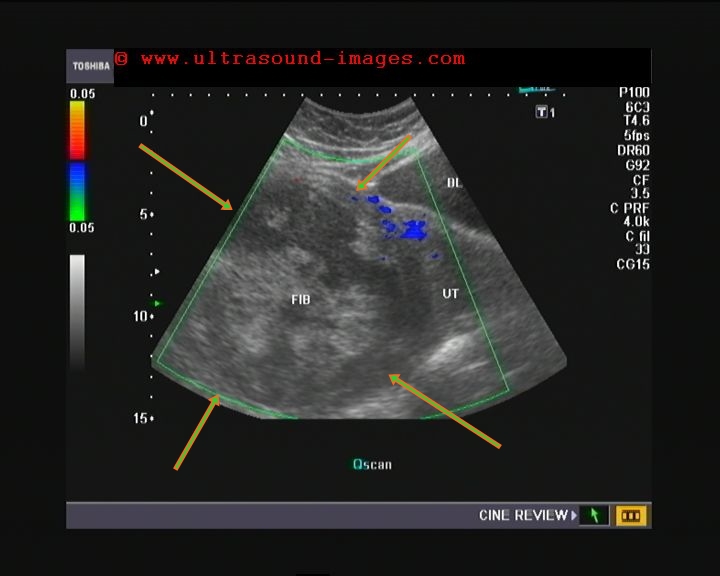
Case-3: Pregnancy with cervical fibroid

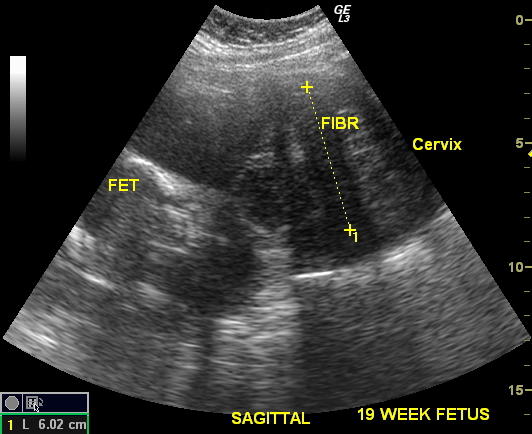

This was a 19 week old pregnancy with the fetus seen to the left of the images. The ultrasound images show a large fibroid involving the lower uterine segment and cervix of the uterus. The mass measures 6 x 7 cms. approximately. Color Doppler image shows poor vascularity of the tumor. (FIBR= fibroid; fet= fetus; BL= bladder).
For more/ ultrasound video clips of this case see:
http://cochinblogs.blogspot.com/2010/05/fibroid-of-cervix-in-19-week-pregnancy.html
Types of fibroid

Download my ebook: sonography of uterine fibroids By Joe Antony, MD)
Read on free Amazon Kindle app or Kindle reader
Sonography of uterine fibroids
For other countries:
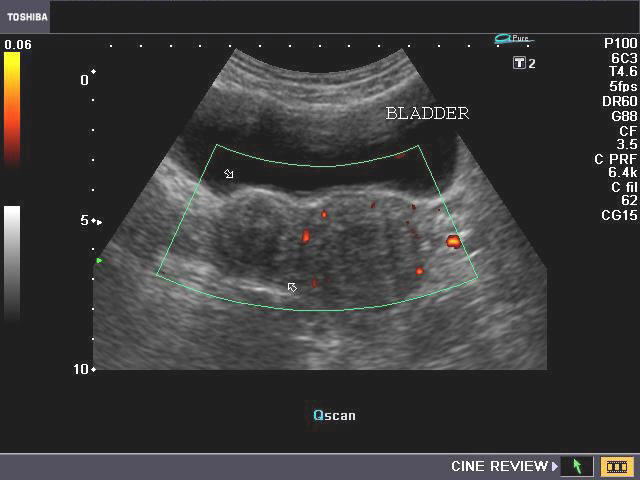
A) Submucous fibroid

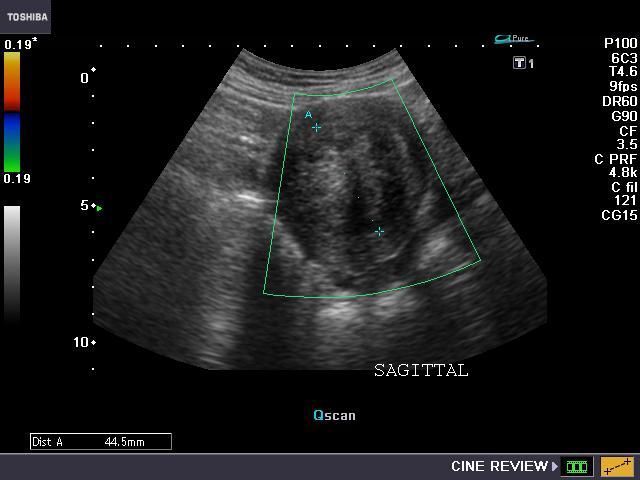

This young adult female patient showed a large hyperechoic well defined, solid mass inside the body of uterus, in close relation to the endometrial cavity. Sonography of the uterus shows that the mass is possibly within the endomterial cavity. Power Doppler image (top-right) shows that there is a rim of vascularity around the mass. The mass measures more than 4 cms. in size. These ultrasound findings/ images suggest submucous fibroid of the uterus. The main differential diagnosis in this case is endometrial polyp. However, the larger size (polyps are usually less than 2 cms. in size) and lack of a single vascular pedicle (seen in polyps) suggest submucous fibroid. Images taken using a Toshiba Nemio-XG ultrasound system by Joe Antony, MD, India.
Reference:http://www.jultrasoundmed.org/cgi/reprint/26/7/941 (free article and images).
case-2: Submucous fibroid: (3-D imaging)
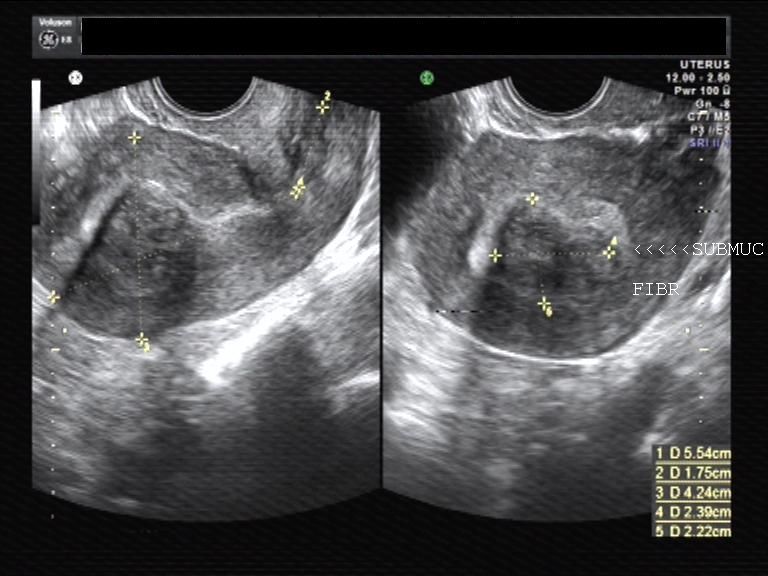

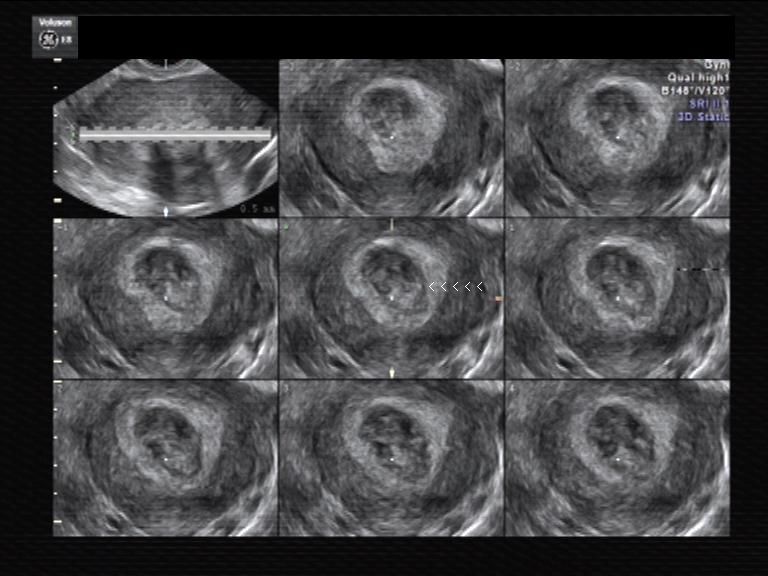

Here are some interesting ultrasound images if a submucous fibroid using a new technique called Volume contrast imaging. This renders 2 D image sections of a volume image (3-D image) acquired of the part being studied (here the Uterus). (Images courtesy of Dr. PK Srivastava, India).
This technique appears to be an application of 3D/ 4D ultrasound. Observe how volume contrast ultrasound images of the uterus bring out the fine detail of the submucous fibroid and its margins. The image on lower right shows the 3-D ultrasound appearance of the disease
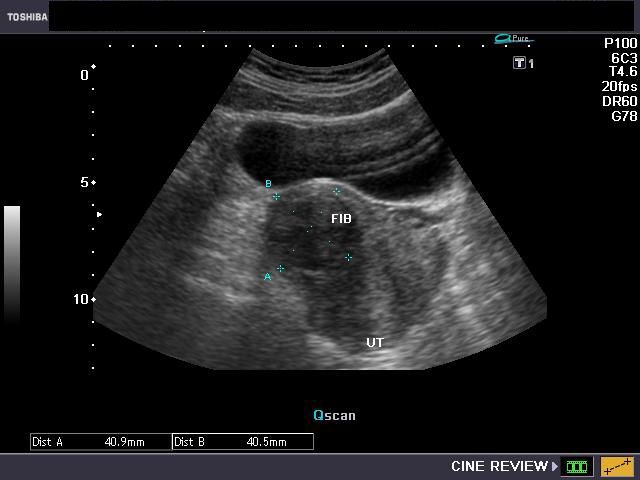
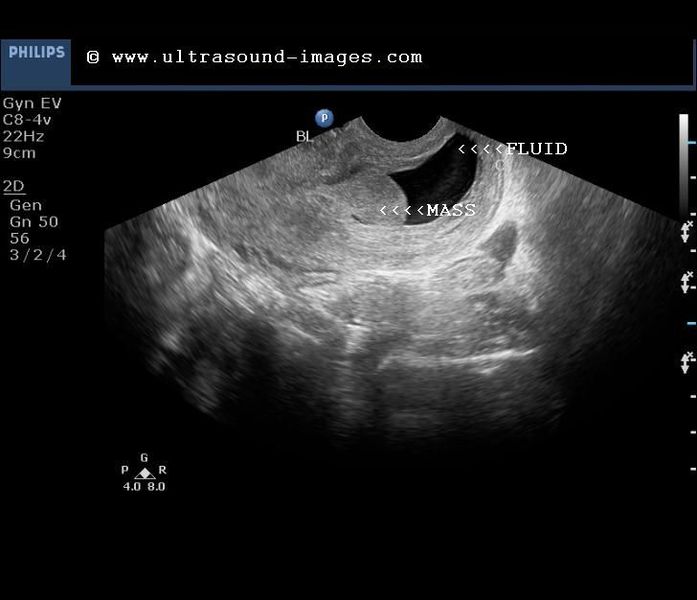
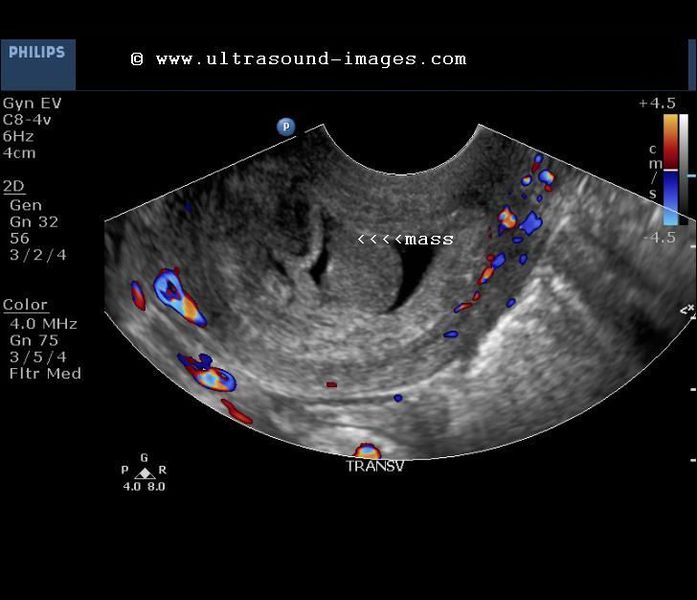
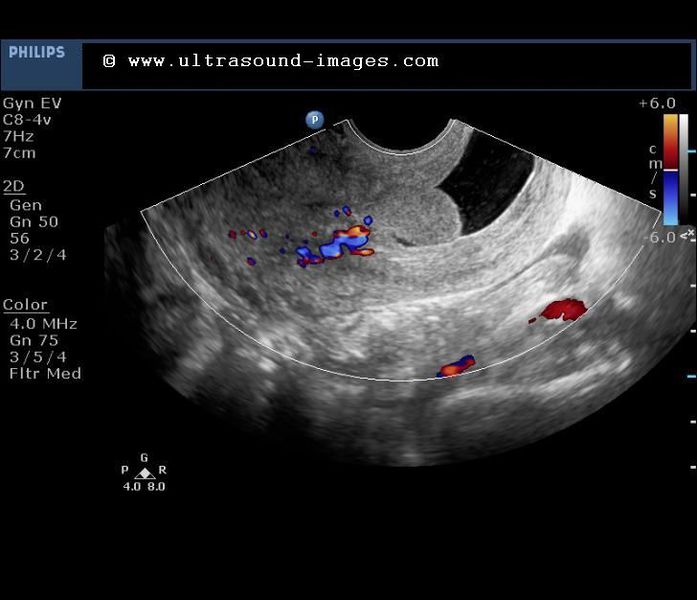
case-3: Submucous fibroid


This was a young adult female patient with a relatively large submucous fibroid bulging into the uterine cavity. Transabdominal ultrasound image (left) shows fluid within the uterine cavity bringing out the mass in contrast. This fluid was naturally present in the endometrial cavity possibly the result of endometritis. Color Doppler image (right) shows vascular pedicle supplying the fibroid. Images are courtesy of Ravi Kadasne, MD, UAE. The machine used here is the Toshiba Aplio.
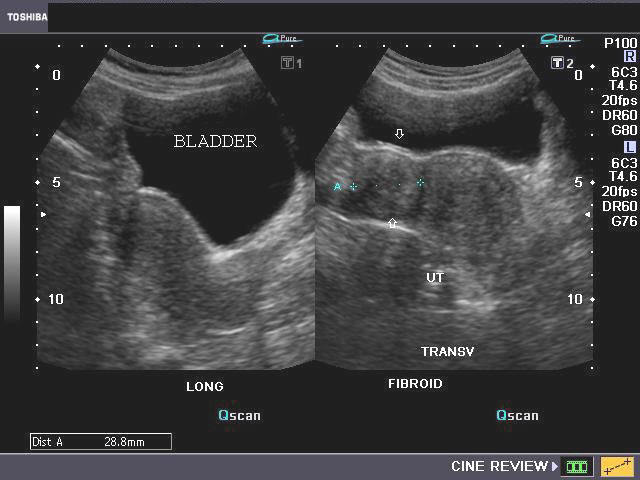
B) Subserosal fibroid (also called Subserous fibroid)

Sonography of the pelvis done on this young adult female patient revealed a large, solid, non-calcific well defined mass located in the anterior wall of the body of uterus. The mass shows absence of central necrosis or infiltration of the bladder wall, though it compresses upon the urinary bladder. Since the mass lies just below the serosal layer of the uterus, these images suggest subserosal fibroid of the uterus. Such large, subserous fibroids of the uterus can cause pain and symptoms due to pressure effect on the urinary bladder, rectum, ureters etc. The Power Doppler image (bottom), shows stretching of the vessels around the rim of the fibroid.
Reference: http://bjr.birjournals.org/cgi/reprint/43/513/602
C) Isthmic fibroid
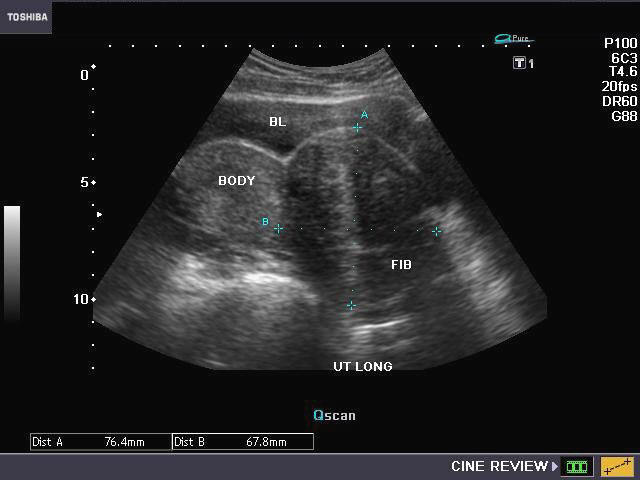
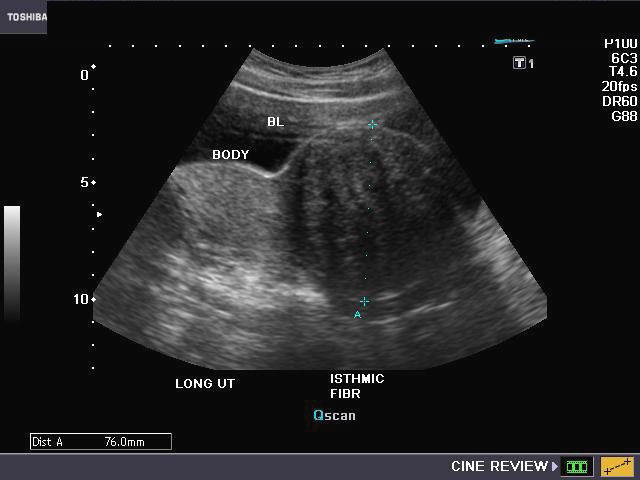
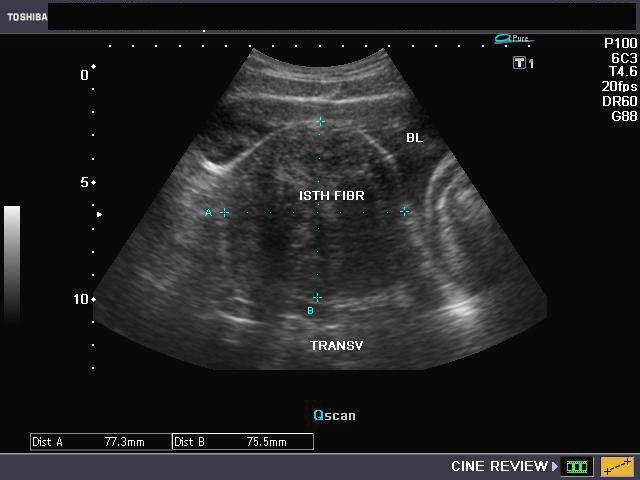
This patient complained of pain in the lower abdomen and was suspected to have a disease of the ovaries or uterus. Sonography of the uterus shows a large, solid mass, 7.5 x 7.7 cms., in the lower part of the uterus, mainly involving the isthmic region (the junction between the body and cervix of the uterus). The mass shows typical features of in intramural fibroid of the uterus. Diagnosis: isthmic fibroid of the uterus. Isthmic fibroids can cause infertility and repeated abortions. Power Doppler image shows the vessels curving around the isthmic mass. Ultrasound images of isthmic fibroid taken using a Nemio-XG ultrasound system by Joe Antony, MD.
D) Broad ligament fibroid
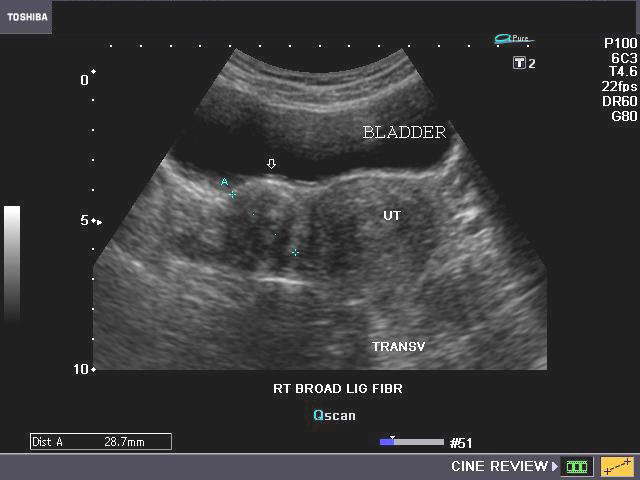
Interligamentous fibroid or fibroid within broad ligament
Sometimes a fibroid can grow laterally into the region between the two layers of the broad ligament, These ultrasound images show a solid mass to the right of the body of uterus. The mass is non calcific and shows no degenerative changes and appears to occupy the right broad ligament (arrows). This suggests a right broad ligament fibroid (also called interligamentous fibroid). Such fibroids can be difficult to remove surgically due to the vessels passing through the broad ligament.
Reference:
1) http://www.healthsquare.com/fgwh/wh1ch07.htm(free article)
2) ://www.jkscience.org/archive/vol8a/BroadLigament.pdf (free article)
E) Broad ligament fibroid with calcification

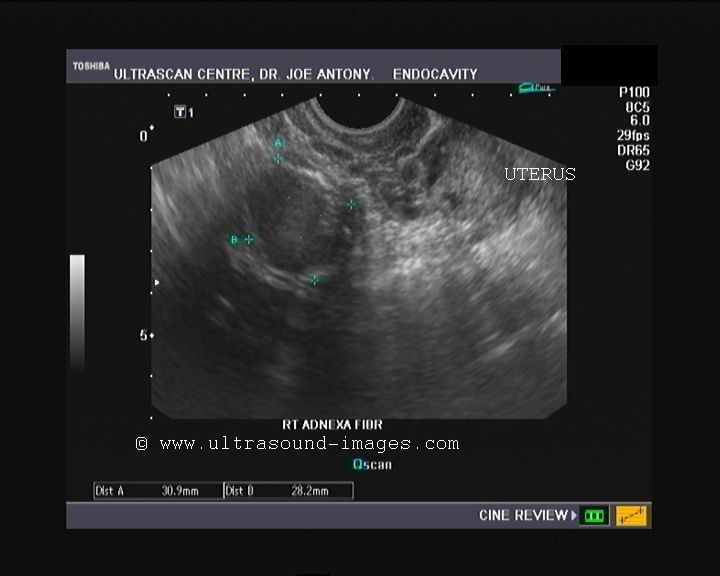
Transabdominal ultrasound Transvaginal ultrasound
This patient was a young lady with pelvic pain. Ultrasound images show-
The transabdominal ultrasound clearly shows a rounded calcific mass (along the rim), in right adnexal region. transvaginal sonography confirms the finding. The transvaginal ultrasound appears more accurate in measuring the size of the calcific broad ligament fibroid (3 cms.). But there is more.....
This image (transabdominal) shows a cystic area anteriorly.
The transvaginal image


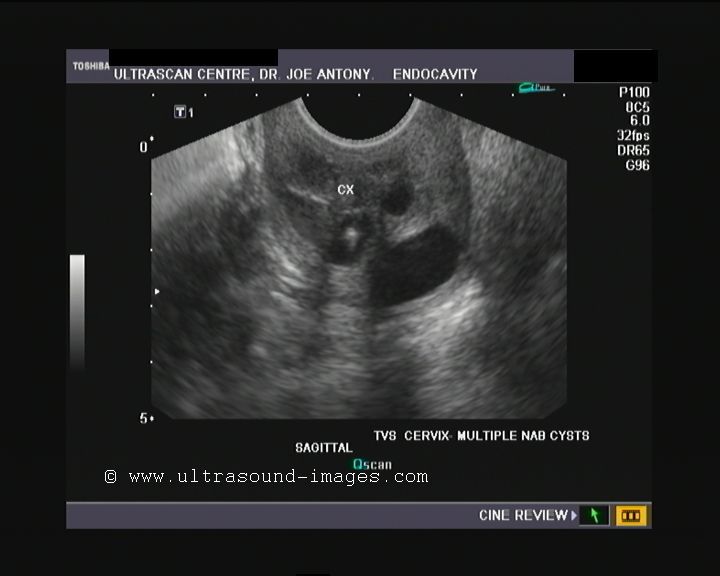
The transabdominal ultrasound image shows a cystic lesion anterior to the uterus. The question- is this a cystic mass? And where does it arise from? The transvaginal image shows this to the cervix with multiple Nabothian cysts studding it. The uterus is markedly retroflexed and retroverted, causing the posterior surfaces of the fundus and the cervix to appose each other. The retroflexion is so severe that the anterior surface of the body of uterus faces posteriorly with the fundus lying posterior to the cervix! This was the cause of the diagnostic dilemma.
The cervix with multiple Nabothian cysts



Fibroids can undergo various degenerative changes, especially when large. This fibroid of the uterus measures 11.2 cms. and shows multiple hypoechoic and hyperechoic patchy areas
Color and Power Doppler images
here is little vascularity within the huge tumor of the upper uterus (fundus and body). Degenerative changes can take place in fibroids with areas of necrosis and hemorrhage and result in varying appearances from cystic to inhomogenous appearances. In fact, it may be difficult to differentiate a large complicated ovarian cyst from a degenerated fibroid.
References:http://www.jultrasoundmed.org/cgi/content/long/25/5/671
Pyometra


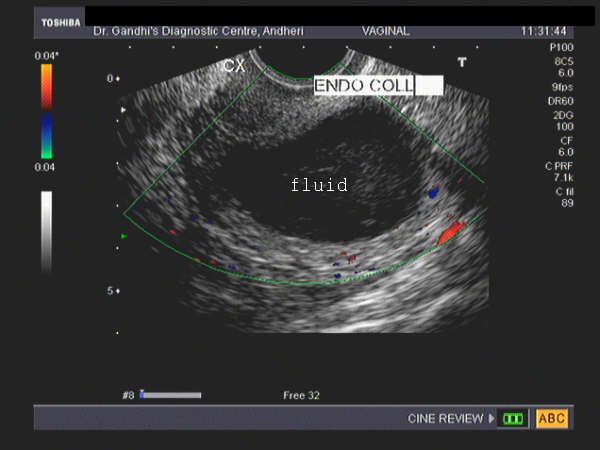
This 70 yr. old patient presented with foul smelling vaginal discharge with fever. Sonography revealed a large collecion of fluid with echogenic debris within the endometrial cavity. Transvaginal ultrasound scan images reveal fluid within the fundus and body in the uterine cavity. These findings are diagnostic of pyometra. Color doppler imaging shows marginal increase in vascularity in the uterine walls. Images courtesy of Dr. Jaydeep Gandhi, Mumbai, India.
Reference:
1) Pyometra What is its clinical significance?abstract- free)
2) Spontaneous Perforation of Pyometra (full text article- free)
Infections of the uterus

Endometritis This female patient presented with symptoms of pelvic inflammatory disease (PID). Sonography of the uterus showed a bulky uterus with fluid distended (possibly purulent) endometrial cavity. The endometrium also appears thickened and hyperechoic. This ultrasound image is diagnostic of endometritis. The commonest of causes of endometritis are Chlamydial and/ or streptococcal infections. Untreated, it may progress to salpingitis or Pelvic abscess. Endometritis is a common disease during immediate post partum period. Ultrasound image is courtesy of Dr. Gunjan Puri, MD, India.
Reference:http://emedicine.medscape.com/article/254169-overview (free article and images).
Migrated IUCD
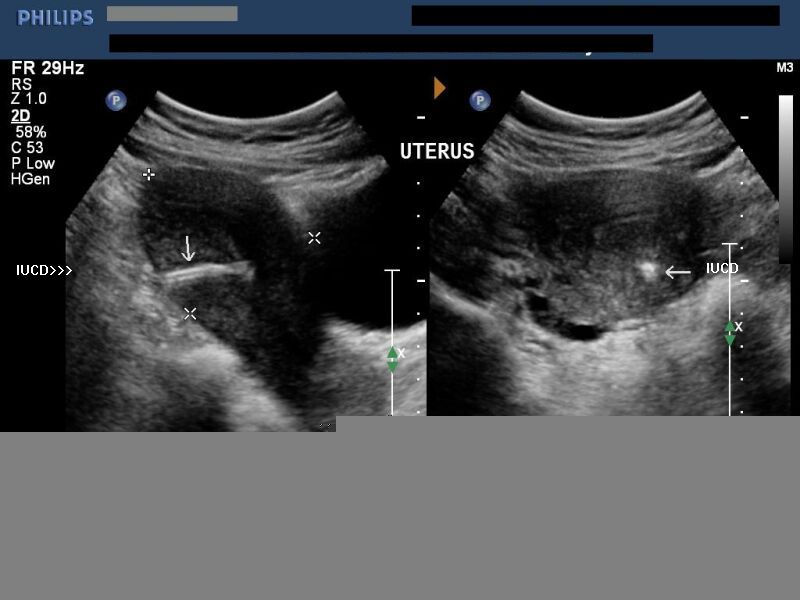
This ultrasound image shows an IUCD (or Intra-uterine contraceptive device) that has migrated from the uterine cavity to pierce the posterior myometrial wall of the body of the uterus. Migration of the IUCD is a known complication of this device. Ultrasound image taken by Dr. Ravi Kadasne, UAE, using a Philips IU-22 ultrasound system.
Reference: http://www.ifpa.ie/contraception/iucd.html (free article)
Congenital anomalies of uterus
Uterus didelphys or Didelphic uterus
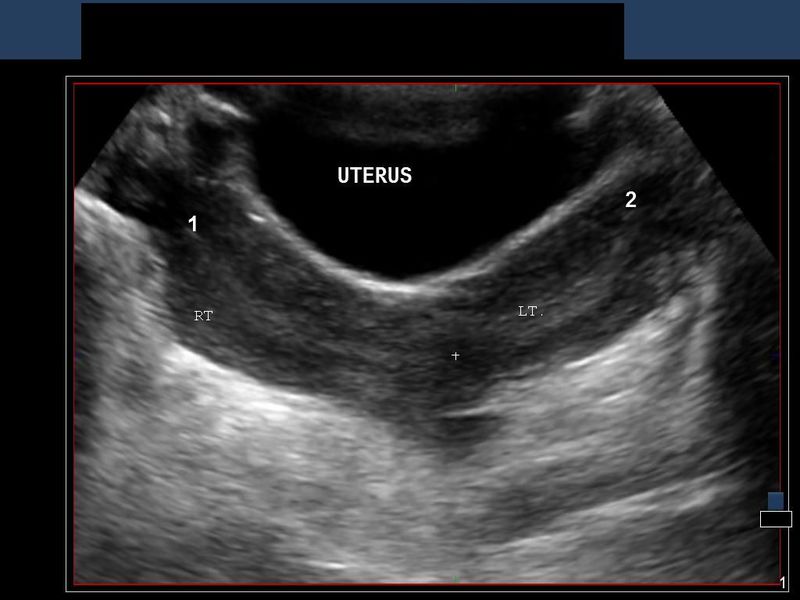
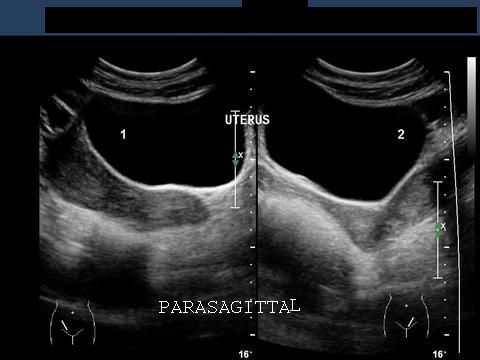

Sonography of the uterus shows 2 separate uteri, 2 separate cervices and separate vagina in this female patient. These ultrasound images are diagnostic of uterus didelphys or didelphic uterus. This is an extreme example of complete failure of fusion of the 2 halves of the uterus (Mullerian ducts) during the fetal stage.
These ultrasound images were taken by Dr. Ravi Kadasne, UAE, using a Philips IU 22 ultrasound machine.
Case-2:
This is a 3D ultrasound image of didelphys uterus. The 3D image again shows separate uterine cavities and separate cervical canals. This 3D ultrasound image of didelphys uterus too is courtesy of Dr. Ravi Kadasne, MD, UAE.
Read more on uterine anomalies at:
http://radiology.rsna.org/content/233/1/19.full
Hypoplastic uterus




Rudimentary uterus.
Transabdominal ultrasonography of the pelvis in this 33 yr. old female patient revealed a very small.
Transvaginal ultrasound images show the uterus measuring about 2.5 x 2 x 1 cms., clearly too small for a woman in the 30s. The uterine cavity (endometrial cavity shows minimal fluid within it). Transverse section ultrasound image shows markedly reduced intercornual distance (less than 2 cms.).
The rudimentary Fallopian tubes are visible, but the ovaries appear very small. Clearly this lady appears to have a hypoplastic uterus with very small ovaries. The chances of conception in such a woman are very low or unlikely.
Reference:http://emedicine.medscape.com/article/405335-imaging
Foreign body in cervix of uterus
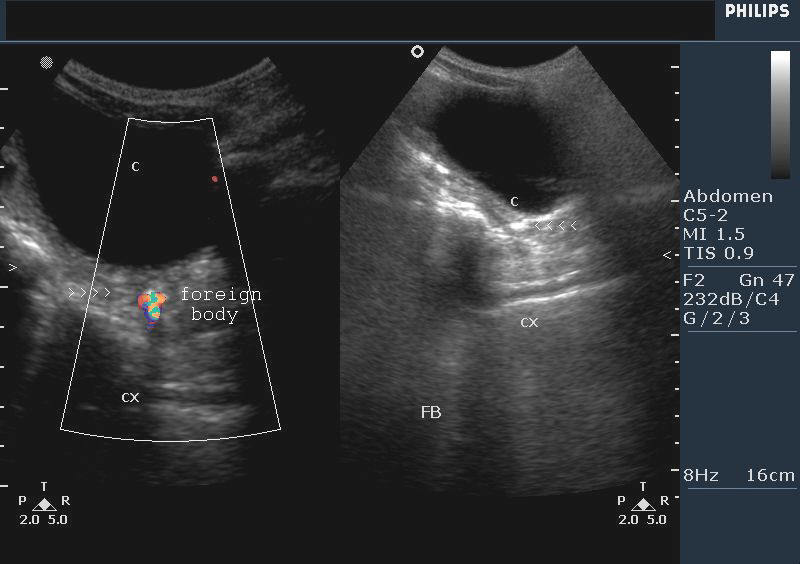
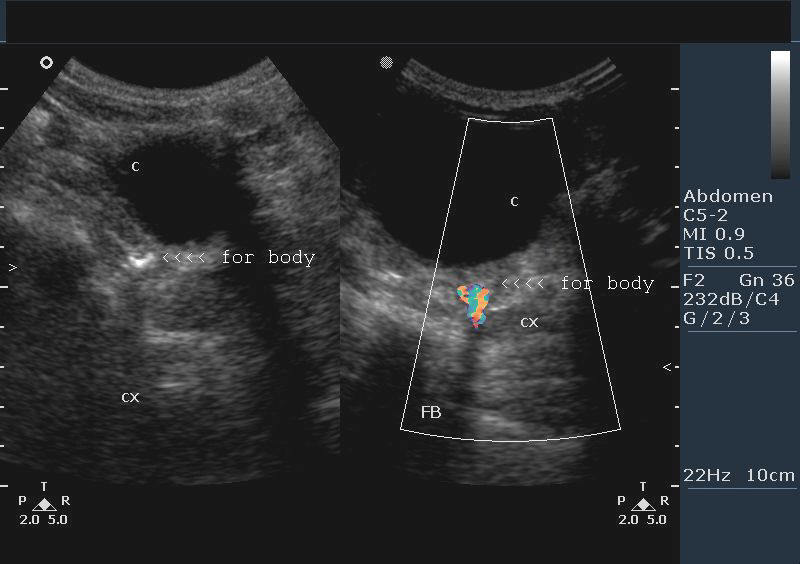


Rice grain in cervix in child
This patient, a 3 yr. old female child had history of sitting and playing on a pile of rice grains. Following this incident, she complained of pain in the pelvis and perineum. Sonography of the pelvis in this child showed an echogenic lesion (echogenic focus) of 4 to 5mm. in the cervix of the uterus. Color Doppler images showed typical twinkling artifact around this lesion. There was intense posterior acoustic shadowing beyond this lesion. Given the history of the child, these ultrasound images suggest foreign body in the cervix, which in this case may be a rice grain. Sonographic images are courtesy of Dr. Vikas Shukla, MD, India.
Reference:http://www.gjms786.com/files/Case%20Vol-6-1.pdf
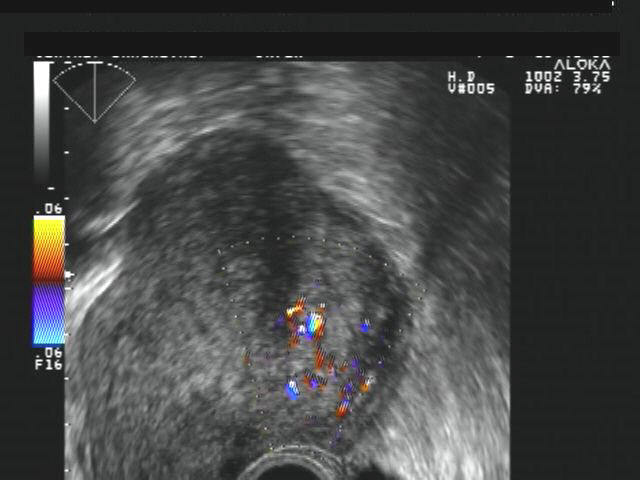
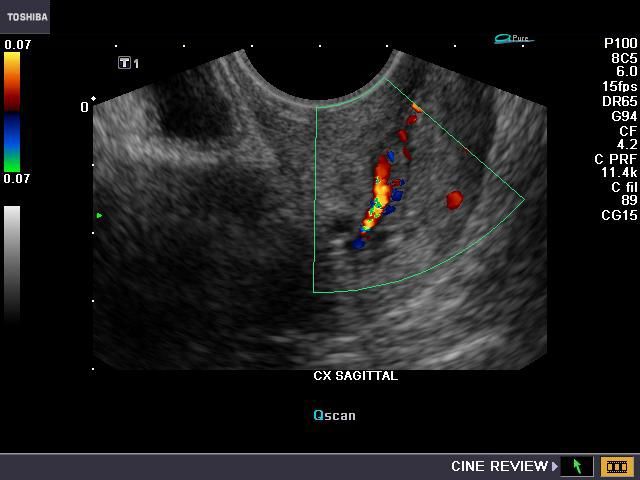
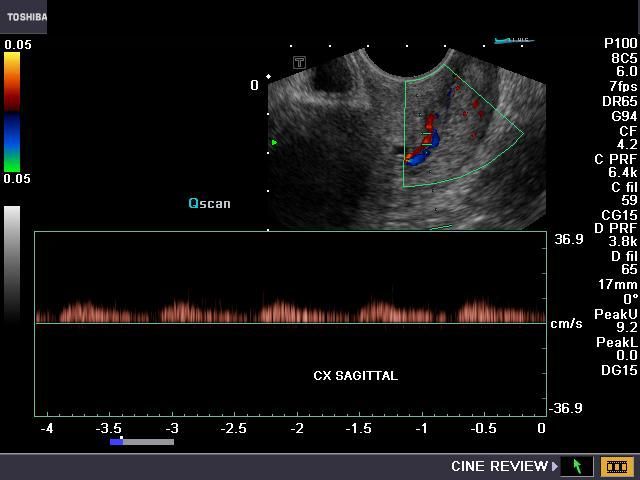
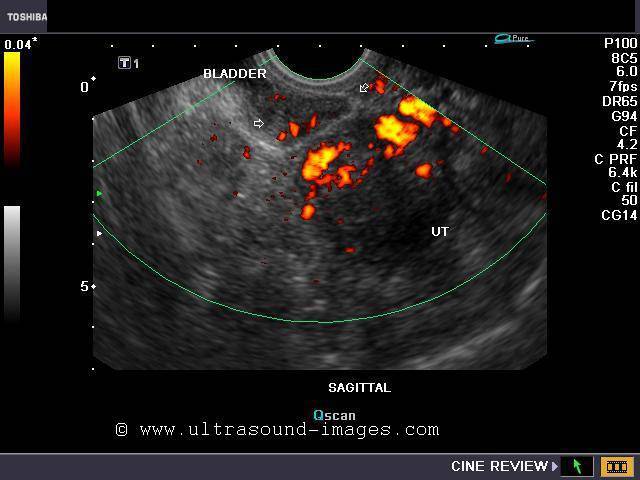
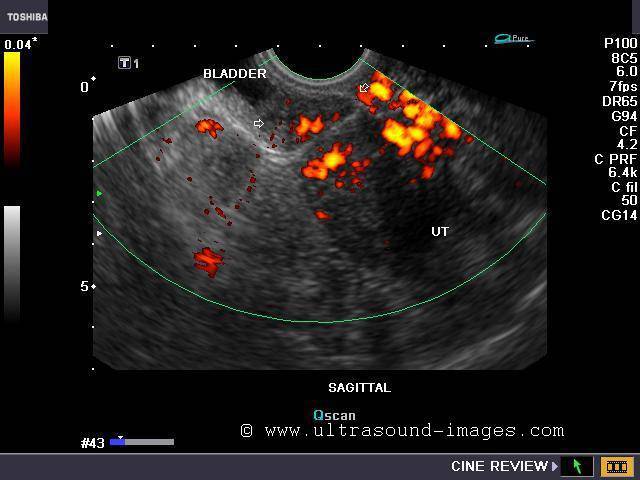
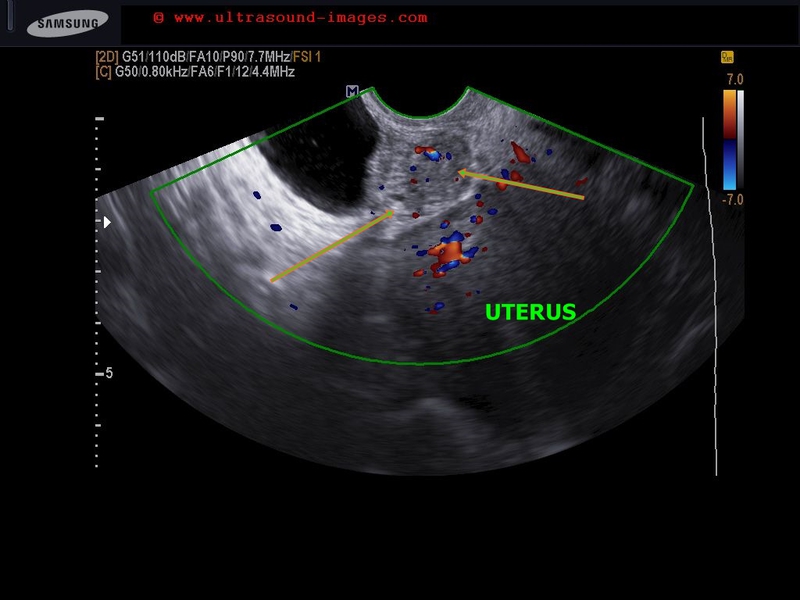
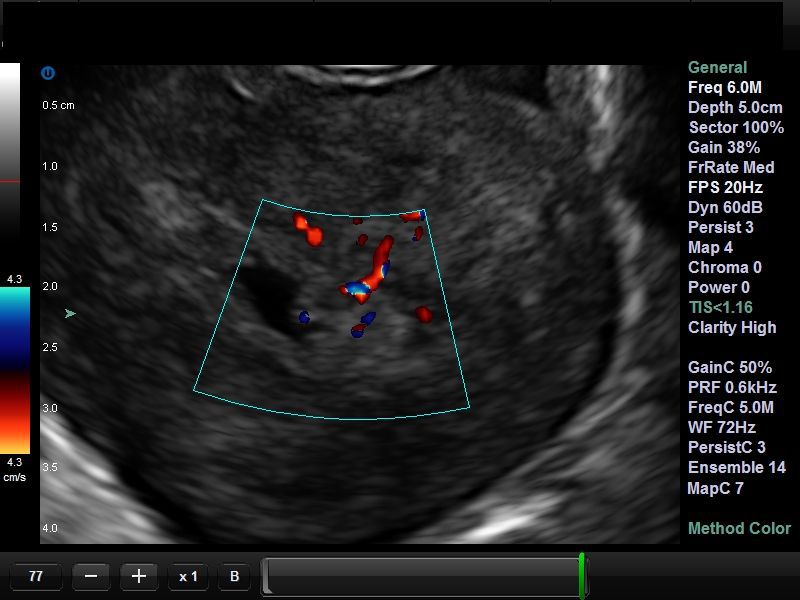
Uterine arterio-venous malformations
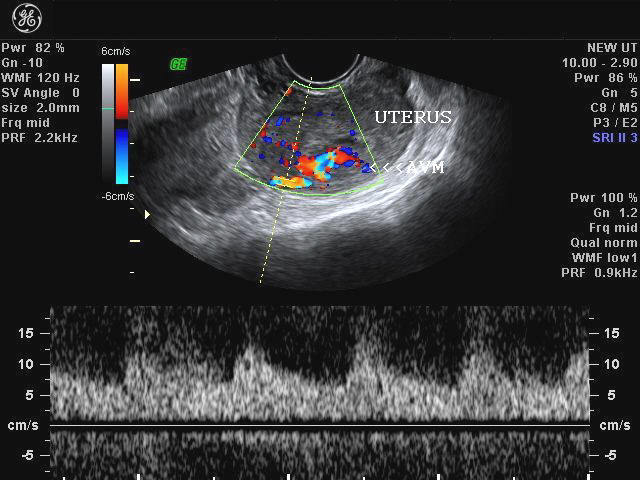
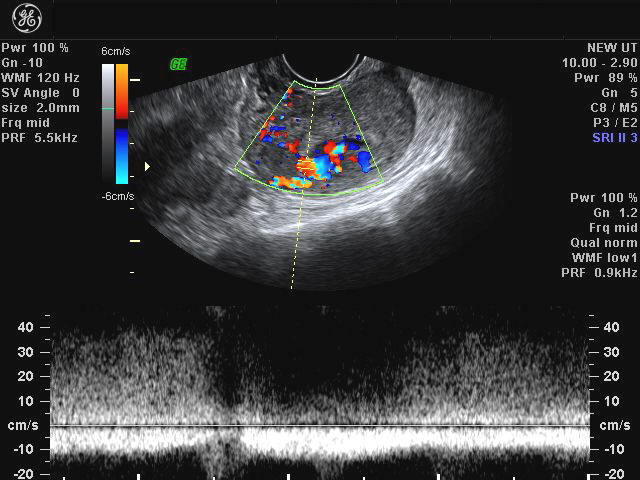
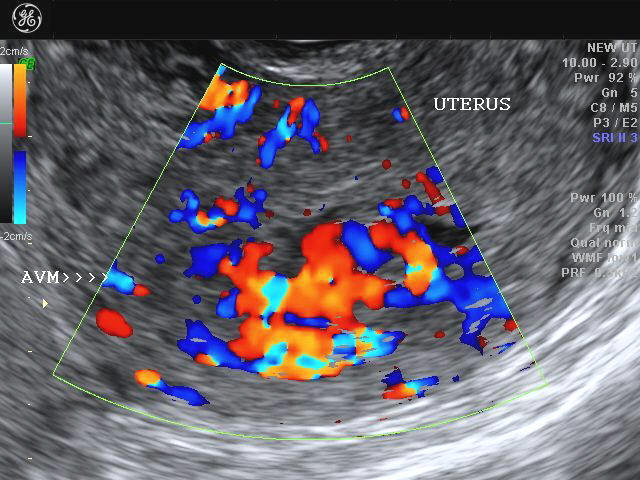
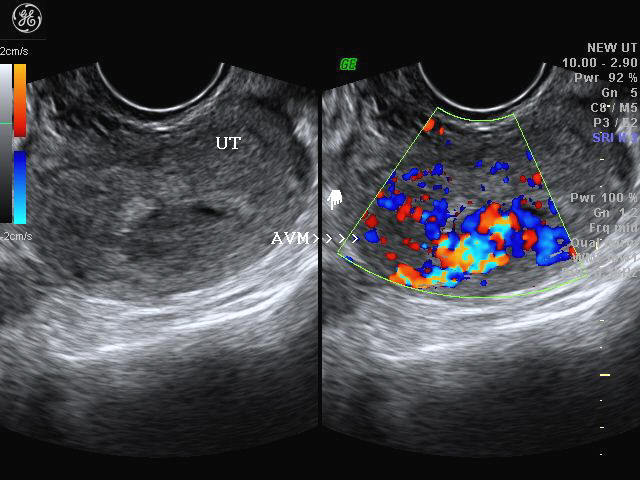
AVM inside the uterus
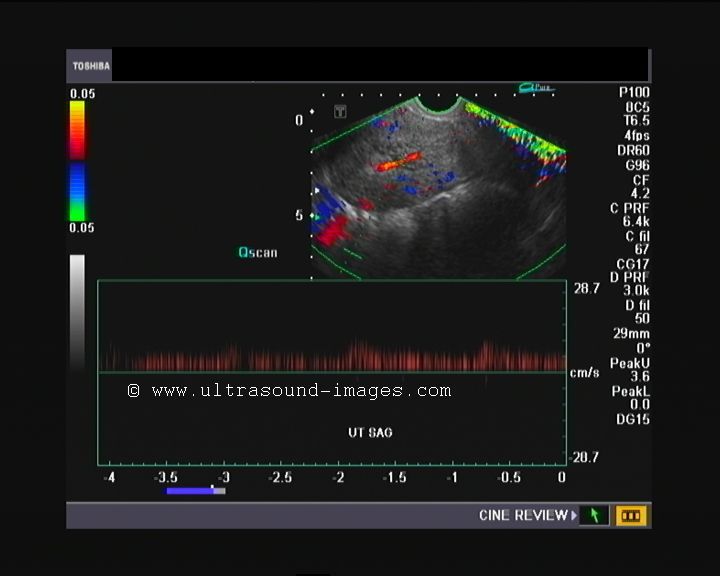
These transvaginal ultrasound and Color Doppler images of the uterus show inhomogenous hypoechoic lesions close to and within the endometrium of this female patient. Color Doppler, in addition, shows a tangle or chaotic pattern multiple dilated vessels in this region of the uterus, extending into its myometrium. Spectral Doppler shows high velocity flow pattern within these vessels, with low resistance (or high diastolic flow). This sonographic appearance is typical of AVM (arterio-venous malformation) of the uterus. This has to differentiated from GTD (gestational trophoblastic disease/ vesicular mole etc.) and retained products of conception. All images are courtesy of Dr. Dilraj Gandhi, MD, India. The machine used here was the GE Voluson.
Reference:
1)http://www.jultrasoundmed.org/cgi/reprint/25/11/1387 (free article and images)
2) http://radiographics.rsna.org/content/22/1/47.full.pdf+html (free article and images)
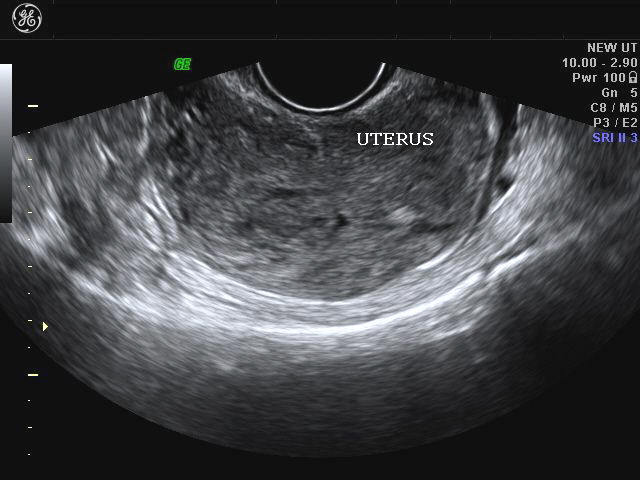
Adenomyosis of uterus

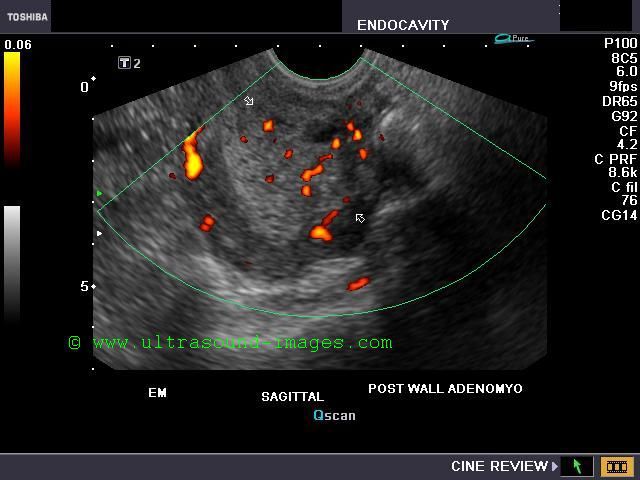
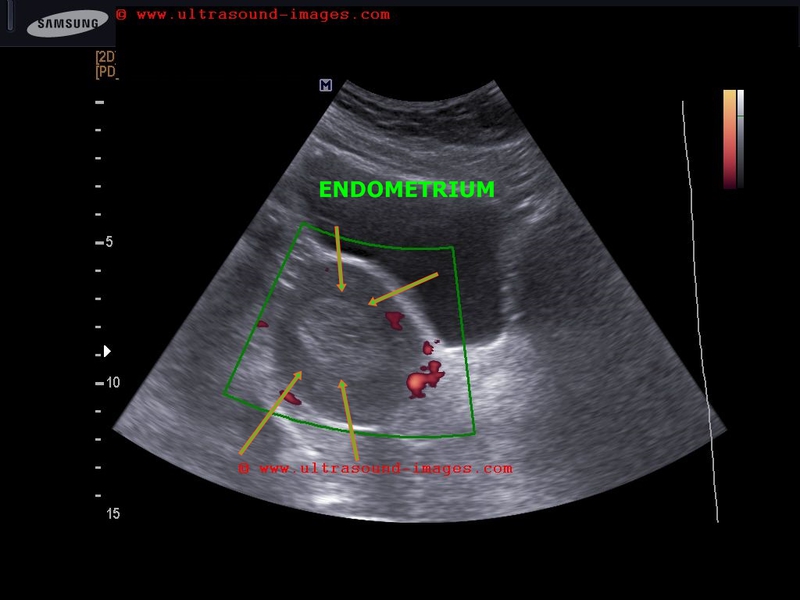
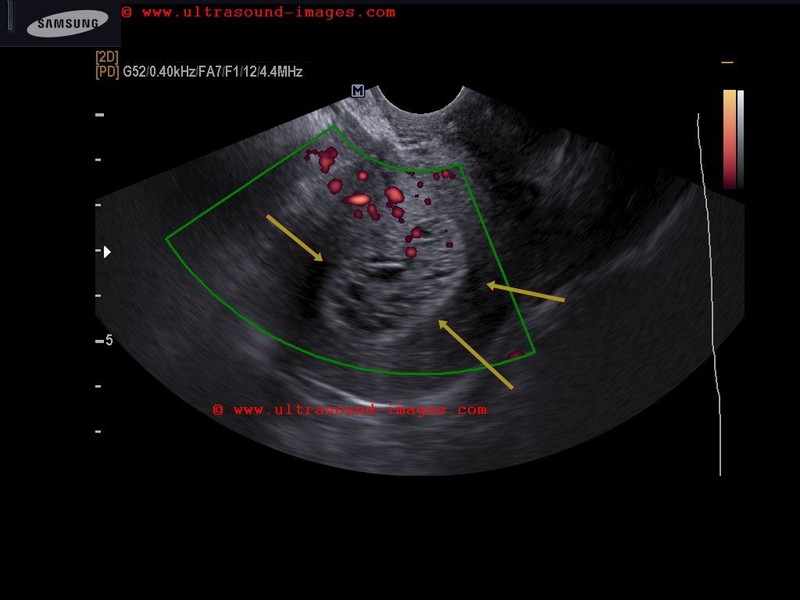
Transvaginal ultrasound and Color Doppler images of the uterus in this patient show: irregular and asymmetric, diffuse enlargement of the uterus, poorly defined myometrial- endometrial interface (poorly defined endometrium), inhomogenous myometrium, streaky acoustic shadowing posterior to the uterus and irregular inhomogenous increase in vascularity of the myometrium (see Color Doppler image of uterus on right). There is also a poorly defined hypoechoic mass in the posterior myometrium. These ultrasound findings are suggestive of adenomyosis of the uterus. Sometimes hypoechoic/ anechoic cystic areas may also be seen in the myometrium in this disease (not seen here). The main differential diagnosis in this case is fibroid of the uterus. However, fibroids are well defined, more or less homogenous masses and do not produce streaky (dirty) shadows. Also, on transvaginal sonography fibroids are usually non-tender on probe pressure. Fibroids also usually have a hypoechoic halo or margin due to compressed vessels. Adenomyosis never contains calcific areas. Ultrasound images are courtesy of Dr. Latha Natarajan, India.
Reference: http://www.medscape.com/viewarticle/459772(free article)
Case-2: Adenomyosis
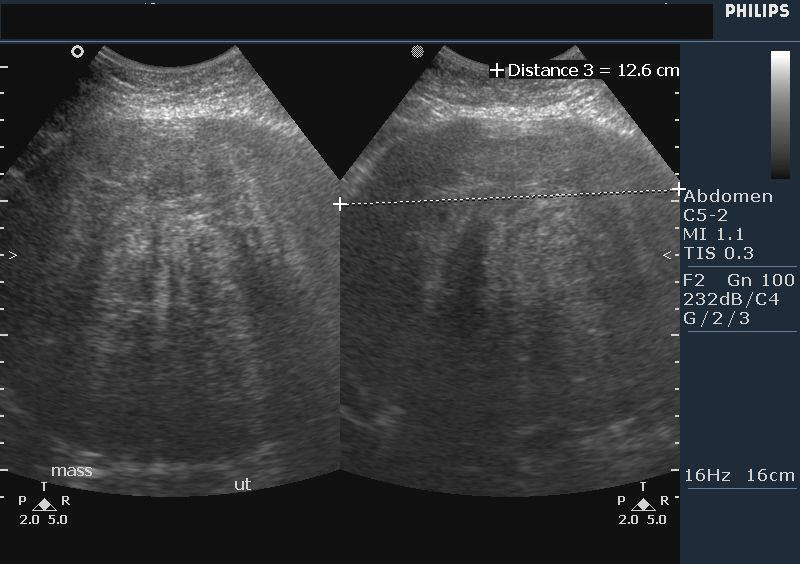
This transabdominal ultrasound image shows a large (bulky) uterus with a diffusely infiltrative, inhomogenous appearance of the myometrium with dirty, streaky shadowing posteriorly. The uterus shows a globular shape with the endometrium almost obscured. These features are typically seen in adenomyosis. However, both fibroids/ leiomyoma of the uterus can simultaneously be present with diffuse adenomyosis as in this case. Ultrasound image courtesy of Vikas Shukla, MD, India.
Case-3: Adenomyosis


This young lady has a history of severe pain during menses. Transvaginal ultrasound imaging shows a simple cyst of the left ovary. The uterus appears bulky with thickened endometrium (12 to 14 mm.). In addition, there is a hyperechoic, inhomogenous lesion posterior to the endometrium and compressing upon it. This lesion also shows some cystic areas within it. Cystic lesions are also present in the endometrium. Myometrial cysts and cystic lesions are characteristic of adenomyosis of the uterus. The hyperechoic myometrial areas are caused by the migration of endometrial tissue into the myometrium. The hypoechoic areas within the adenomyotic lesions are the result of hyperplasia of the myometrial smooth muscle around the ectopic endometrial tissue. The actual measure of the adenomyosis being hypoechoic or hyperechoic depends on the ratio of smooth muscle hyperplasia (hypoechoic) to the endometrial tissue (hyperechoic) within the lesion in the myometrium.

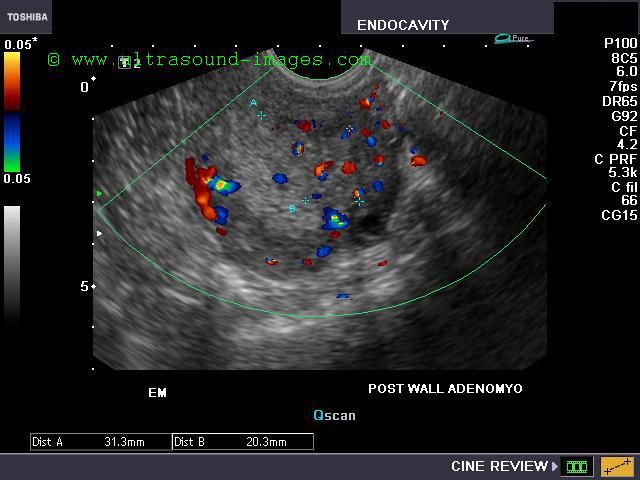

The above color Doppler and Power Doppler images further confirm the highly vascular nature of the lesion. These ultrasound appearances are diagnostic of adenomyosis of the uterus. The left ovarian cyst was just an incidental finding, but not the cause of dysmenorrhea.
Color Doppler videos of this case are at:
http://ultrasound-videos.blogspot.com/2011/03/adenomyosis-of-uterus.html
http://radiographics.rsna.org/content/19/suppl_1/S147.full
http://www.ajronline.org/content/179/2/379.full
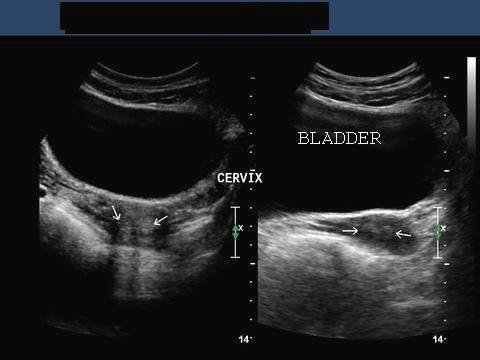
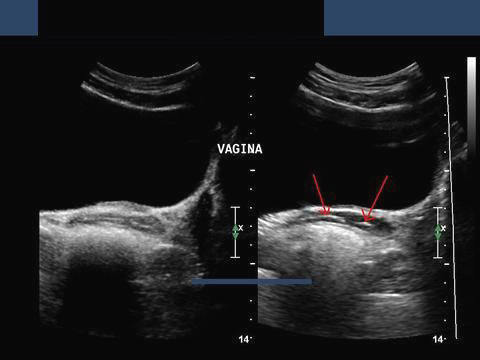
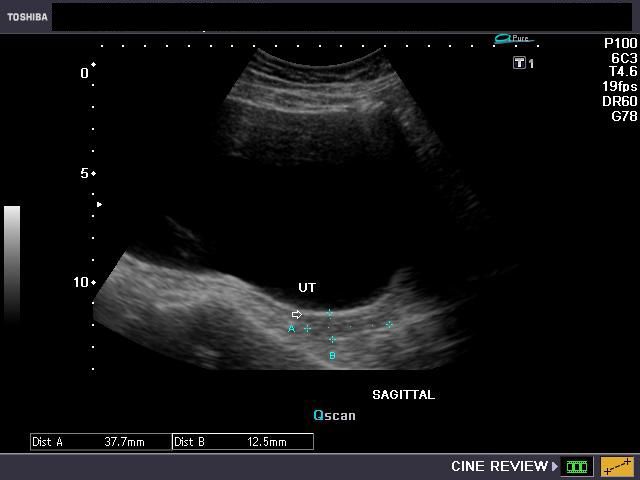
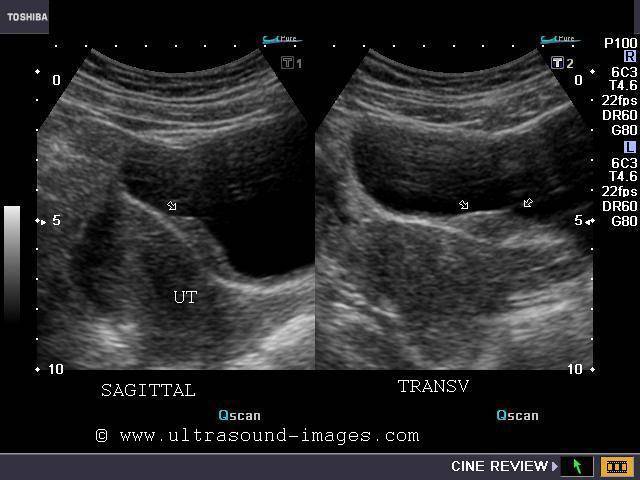
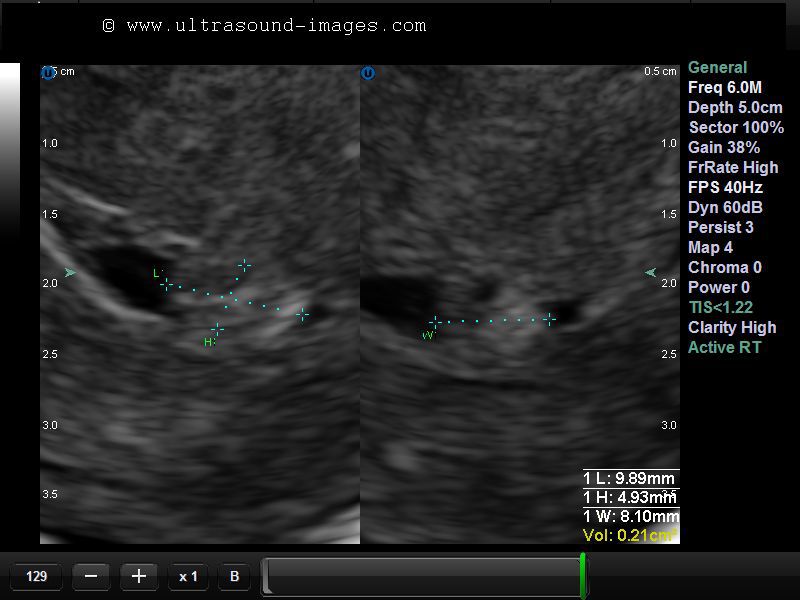
Asherman's syndrome: Uterine synechiae

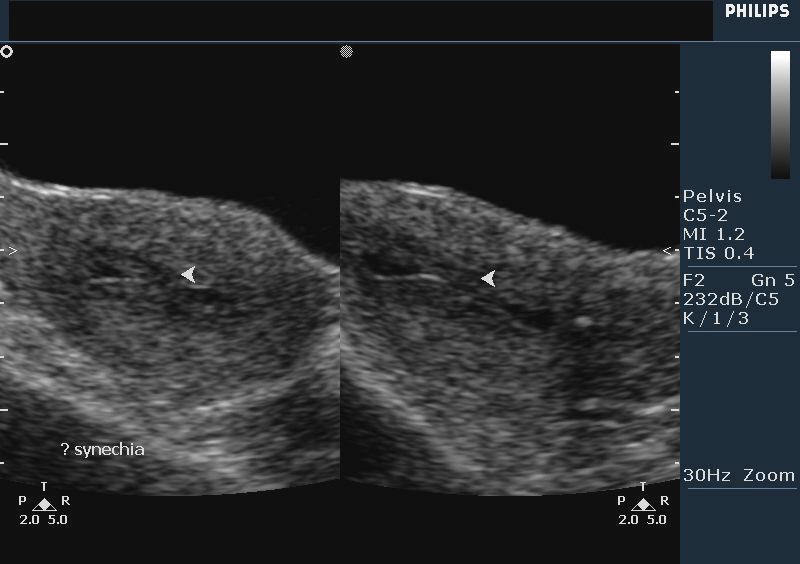
This young adult female patient underwent D &C (dilatation and curettage) some time ago. Presently, she presented with abdominal pain. The sagittal ultrasound images of the uterus show small amount of fluid inside the endometrial cavity with adhesions between the anterior and posterior walls of the cavity (arrowheads). These ultrasound findings are diagnostic of Asherman's syndrome or uterine synechia/ adhesions. Synechiae of the uterus are typically seen following a D & C of the uterus. The cause is possibly adhesions or scarring within the walls of the raw surfaces of the uterine cavity. This condition is usually treated by surgical intervention, using a procedure called adhesiolysis during hysteroscopy. Untreated, this condition can result in infertility and amenorrhea. Ultrasound images are courtesy of Dr. Vikas Shukla, MD, India.
Reference:
http://en.wikipedia.org/wiki/Asherman%27s_syndrome
http://pjms.com.pk/issues/octdec05/article/article13.html
Pedunculated polyp of the cervix

Transabdominal ultrasound scan in this middle aged lady showed a bulky uterus with a small hypoechoic lesion in the anterior wall of the fundus. Possibly, this is a cases of adenomyosis of the uterus. But, this alone did not appear to explain the cause of her symptoms. Transvaginal ultrasound images revealed a cervical pathology
Grey scale images

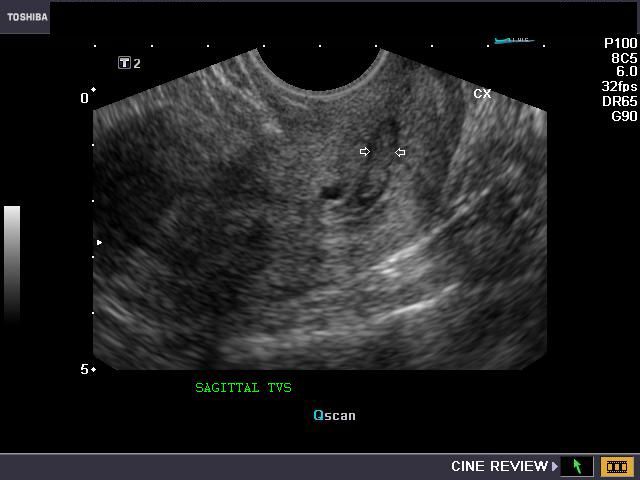
Transvaginal ultrasound images of the cervix (sagittal) show a 6 x 15 mm. long, echogenic mass in the endocervical canal. The diagnostic possibilities here appear to be prolapsed endometrial polyp (descending from the uterine cavity above) or a small endocervical fibroid. However, there appeared to be no extension of the mass upwards, with its boundaries, well within the endocervix. Transvaginal color Doppler ultrasound images in both sagittal and transverse sections revealed:
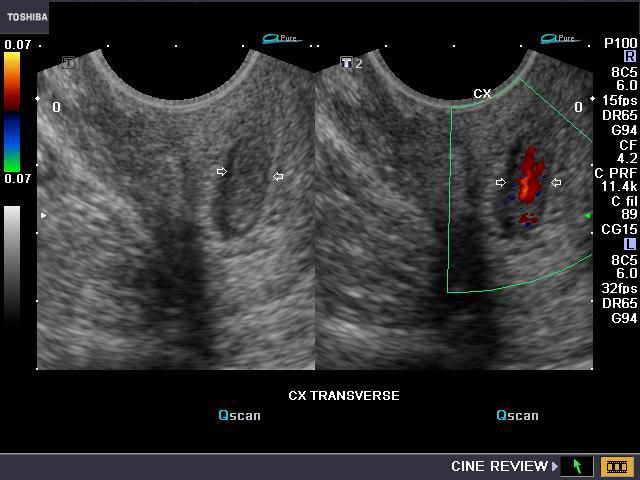
Clearly this is a very vascular fleshy mass within the endocervix, the most probable diagnosis being a cervica, pedunculated polyp
Power doppler and Spectral Doppler trace images

There is pulsatile flow within the vessels in the cervical canal, further confirming the highly vascular nature of the mass. Final diagnosis - pedunculated polyp of the cervix.
Ultrasound video showing the cervical polyp (below):
Reference:
http://onlinelibrary.wiley.com/doi/10.1002/uog.1992/pdf (free article and images).
For a color Doppler ultrasound video demonstration of this case see:
http://ultrasound-videos.blogspot.com/2010/11/pedunculated-cervical-polyp-ultrasound.html
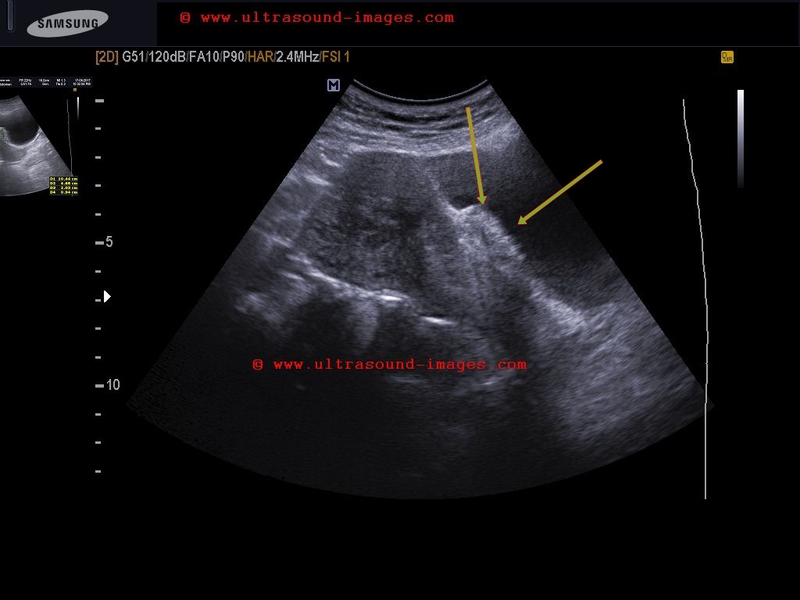
Pedunculated fibroid of the cervix
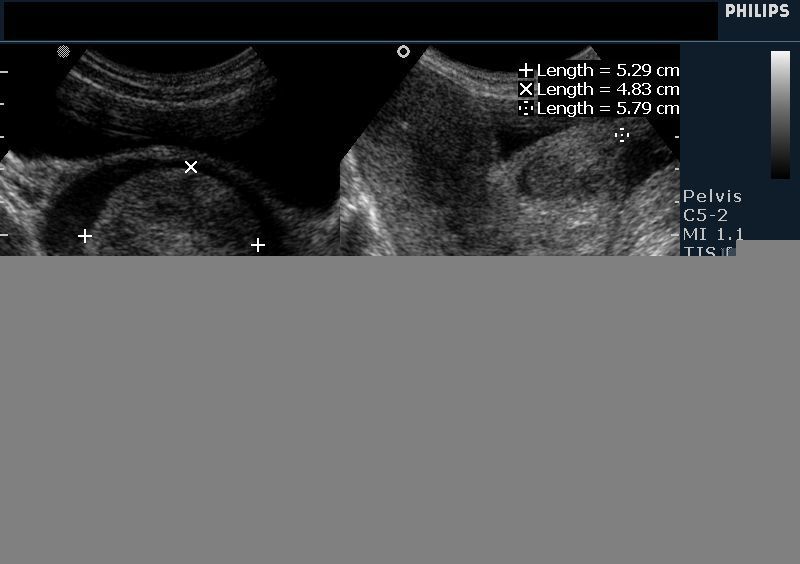
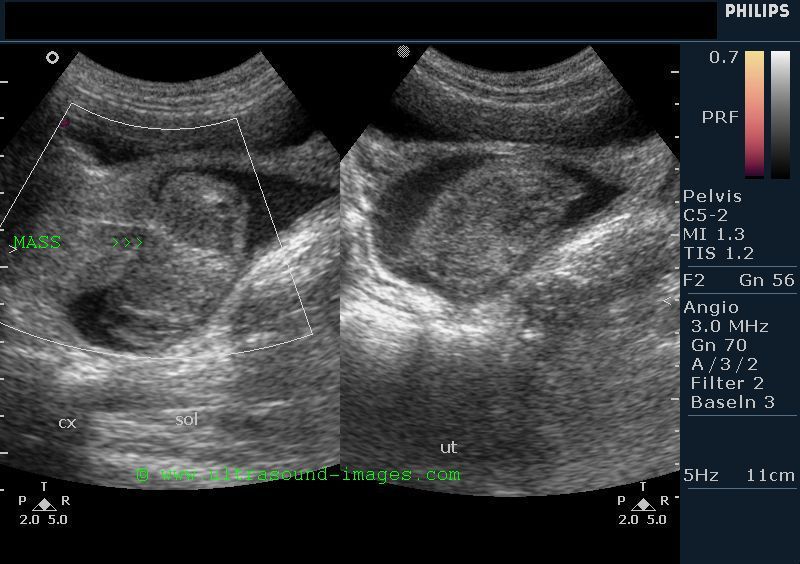
This lady has a large mass in the endocervical canal (measuring 5.3 x 5.8 cms.). The mass is solid and inhomogenous, well outlined by fluid surrounding the tumor. This mass is well defined in outline with a short peduncle (stalk) connecting it to the endocervix. These ultrasound images suggest pedunculated fibroid of the cervix. The large size differentiates this mass from a polyp of the cervix (see case 13 above). Ultrasound images are courtesy of Dr. Vikas Shukla, MD, India.
References: http://emedicine.medscape.com/article/405676-overview
Case-2: Pedunculated fibroid of cervix


This is yet another case of a large pedunculated mass in the cervix or to be more precise in the endocervical canal. The mass measures 1.2 cm in size and projects into the endocervical canal from above. This is the typical appearance of a pedunculated fibroid or possibly a large polyp descending from the uterine cavity above. Again, it is the large size of the mass projecting into the endocervical canal that favors a diagnosis of pedunculated fibroid rather than a pedunculated polyp of the cervix. Of the two images above, the transabdominal ultrasound image on the left shows a sagittal section of the uterus clearly displaying the polypoid mass descending into the cervix.
Transvaginal ultrasound images
Two of the transvaginal ultrasound images above show colour Doppler study of the uterus displaying vessels leading to the polypoid mass. Again, the limited vascularity of the mass suggests a diagnosis of pedunculated fibroid ( submucosal), rather than a diagnosis of the pedunculated polyp of the cervix. another striking feature of these ultrasound images is the presence of fluid within the endocervical canal. This appearance is also seen in the earlier case and may be caused by stenosis of the outlet of the endocervical canal.
Nabothian cysts of the cervix
Ultrasound image- sagittal section uterus

This 42 year old patient presented with irregular menses and lower abdominal pain. Transvaginal ultrasound shows thickened endometrium, with multiple cystic lesions of the cervix- the largest cyst being 15 mm. in size. Dystrophic calcification is present in one of the cysts in the cervix. The commonest cause of cystic lesions in the cervix is Nabothian follicles or Nabothian cysts. Usually these cysts are 3 to 5 mm. in diameter. In this the Nabothian cysts measure up to 15 mm. in size. Nabothian follicles are also called mucinous retention cysts and are the result of obstruction of the mucous glands of the endocervix resulting in accumulation of mucous within the glands. Unless they are large or multiple or infected they are usually asymptomatic and do not require surgical or medical treatment.
References:
http://radiographics.rsna.org/content/25/1/3.full(free article and images)
http://en.wikipedia.org/wiki/Nabothian_cyst Article in Nabothian cysts
Lipoleiomyoma of uterus

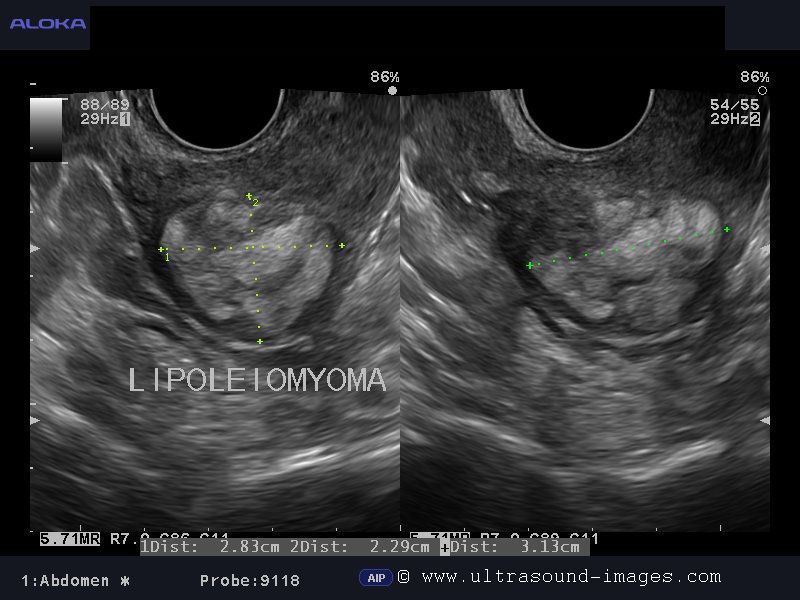
This postmenopausal woman presented with pelvic pain and discomfort. Ultrasound images show a markedly hyperechoic, rounded mass of approximately 3 cms. in the lower part of the body of uterus. The mass is intramural in location and shows a hypoechoic rim around it. These ultrasound imaging characteristics are diagnostic of lipoleiomyoma of the uterus. A small amount of fluid is present in the uterine cavity. So what is a lipoleiomyoma of the uterus? These are benign tumors of the uterus and are typically found in the body of the uterus. Lipoleiomyomas are essentially fibroids of the uterus that have undergone fatty degeneration of the smooth muscle cells within the leiomyoma (fibroid). Thus lipoleiomyomas of the uterus contain smooth muscle, fatty tissue (adipose cells) and fibrous tissue. Ultrasound images of lipoleiomyoma of uterus are courtesy of Dr. Jaydeep Gandhi, MD, India. The machine used here is the Aloka Prosound Alpha 7 ultrasound system.
References:
Free article on radiology of lipoleiomyoma of uterus
AJR article on imaging of lipoleiomyoma of uterus
http://bjr.birjournals.org/cgi/reprint/70/838/1068.pdf(radiology of lipoleiomyoma)
Cystic hyperplasia of endometrium
Sagittal section of the uterus (TV scan ultrasound images)


case-2-cystic hyperplasia of endometrium

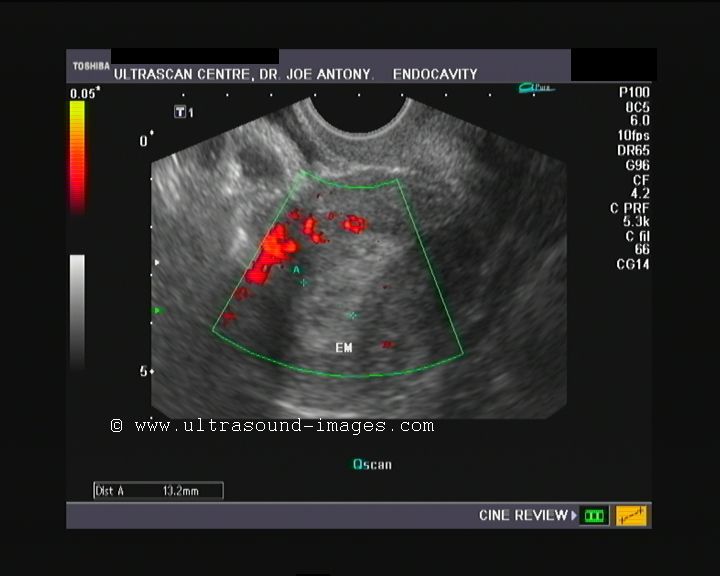
This young 25 year old female patient had polymenorrhea for which she underwent medication using Novex-DS (an estrogen receptor modulator) and regesterone. The endometrium shows typical changes of long term use of estrogen agonists or high estrogenic exposure. Endometrial thickness here measures 20 mm. There is also evidence of minute cysts within the endometrium s/o cystic hyperplasia. If the endometrial thickness exceeds 10mm., it is said to be hyperplastic. Endometrial hyperplasia can be reliably excluded if the endometrial thickness is less than 6 mm. These ultrasound and color Doppler images show cystic endometrial hyperplasia, a condition that is often seen in women who undergo medication with tamoxifen. Endometrial hyperplasia can be classified into- cystic, adenomatous and atypical depending on the ultrasound appearances. There is also a prominent feeder vessel passing through the endometrium in this patient suggesting a differential diagnosis of cystic changes within an endometrial polyp. Such changes of cystic hyperplasia of the endometrium seen in premenopausal women are usually reversible after withdrawal of exposure to the medication.
Case-2:
another example of cystic hyperplasia of endometrium in a 44 yr old lady on treatment for polymenorrhoea.
References:
http://radiographics.rsna.org/content/21/6/1409.full(ultrasound imaging of endometrial hyperplasia)
Endometriosis of urinary bladder


Case-2: 3D ultrasound images of bladder endometriosis

Case-1: (Top)
This 30 year old female patient has a history of endometriosis and has undergone treatment for an endometrioma of the Left ovary. She also has history of pain during micturition. Ultrasound images of the urinary bladder show marked thickening of the posterior wall of the urinary bladder (22 x 7 mm. sized lesion). This area of thickening of the bladder is seen to project into the lumen of the urinary bladder on both transabdominal and transvaginal ultrasound imaging. The lesion also shows marked vascularity in transvaginal color and Power Doppler imaging. The uterus also shows marked vasculrity in the anterior wall adjacent to the bladder lesion. These ultrasound images suggest a diagnosis of endometriosis of the urinary bladder, especially in view of the patient's past history of endometriosis. Endometriosis of the urinary bladder is relatively rare with only an incidence of 3 % of all cases of endometriosis. Surgical removal of the lesion is the only effective treatment. The main differential diagnoses in this case include cystitis giving rise to bladder thickening and also bladder neoplasia including carcinoma of the urinary bladder.
Case-2: (lower set of images): a similar case of urinary bladder endometriosis with invasion of the urinary bladder by endometriotic implant. In addition, there is a fibroid of the uterine fundus. 3D ultrasound images with surface rendering show the lesion clearly abutting the posterior surface of the bladder. This lady complained of dysmenorhoea. The endometriotic lesion was 1st detected 2 years earlier and has reduced in size in the current sonographic study.
References:
1) http://bjr.birjournals.org/content/74/882/556.full
2) AJR article on endometriosis
3) Radiographics article on endometriosis imaging
4) Case report of urinary bladder endometriosis
5) Bladder endometriosis- ultrasound study
Carcinoma of the cervix




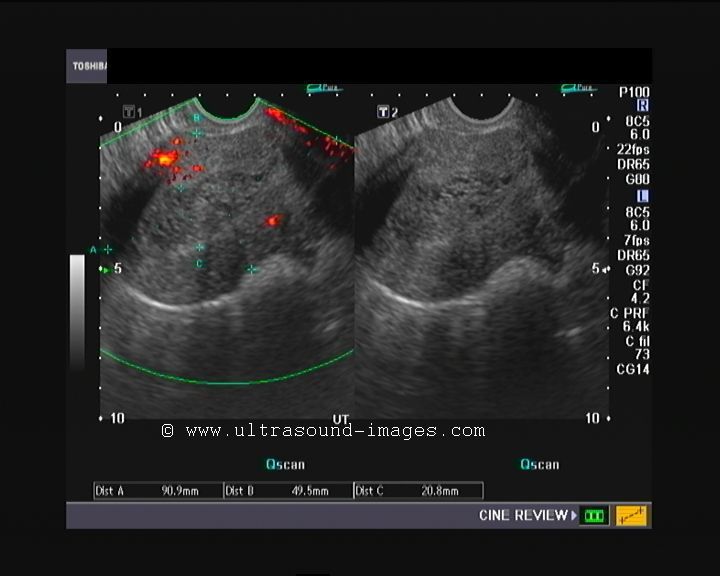
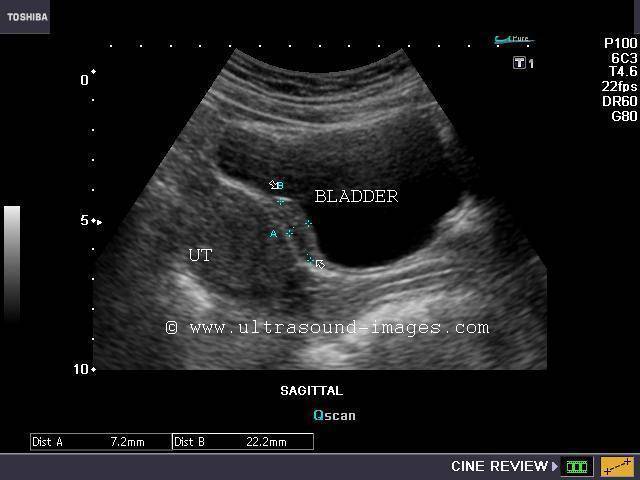
This middle aged lady had vaginal bleeding and discharge. Ultrasound images of the pelvis show an isoechoic mass arising from the cervix invading the posterior wall of the urinary bladder. Color Doppler imaging shows neovascularity of the tumor. The uterus shows a hypoechoic collection within the endometrial cavity suggesting pyometra or hydrometra. 3D ultrasound image shows the mass clearly invading the bladder. These ultrasound images suggest a malignant tumor of the cervix- cervical carcinoma or carcinoma of the cervix with invasion of the bladder. Pyometra is a typical finding in cases of cervical carcinoma and is caused by obstruction of the cervical canal by the cervical tumor. The differential diagnosis in such a case includes bladder endometriosis which can produce a similar appearance. However, there is usually no evidence of pyometra or hydrometra in bladder endometriosis. Another lesion that can mimic a cervical carcinoma is cervical fibroid. Again cervical fibroids would not produce invasion of the bladder. These ultrasound images of carcinoma of cervix are courtesy of Dr. Sanjiv Bhalla, MBBS, Faridkot, India.
References:
article on radiology of carcinoma of the cervix
Ultrasound imaging in carcinoma of the cervix
Endometrial hyperplasia




This post menopausal patient presented with bleeding P/V with discharge per vagina. Ultrasound imaging of the uterus shows a markedly thickened endometrium at 24 mm. There is marked inhomogeneity of the endometrium with a suggestion of endometrial polyp like mass within the endometrial cavity. Medical literature suggests that any endometrial thickness of more than 10 mm. in a post menopausal woman is typical of endometrial hyperplasia. The greater the thickness of the endometrium, the higher are the chances of endometrial carcinoma. Thus this patient shows typical changes of endometrial hyperplasia with a high likelihood of malignancy. The 3D-ultrasound image on bottom row- Right, shows the full extent of the endometrial hyperplasia. Endometrial thickness of less than 6 mm. almost certainly excludes hyerplasia of the endometrium. A close differential diagnosis in this case is endometrial polyp. However, no feeder vessel is seen on color Doppler imaging.
References: Article on endometrial hyperplasia- radiographics
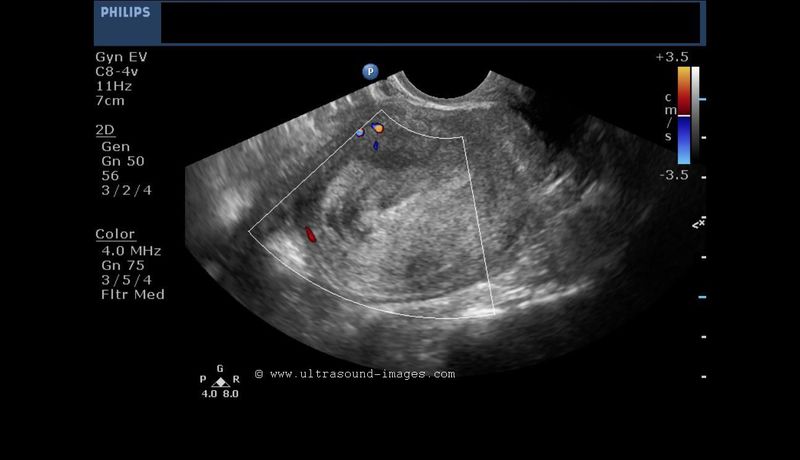
3D-ultrasound images normal uterus
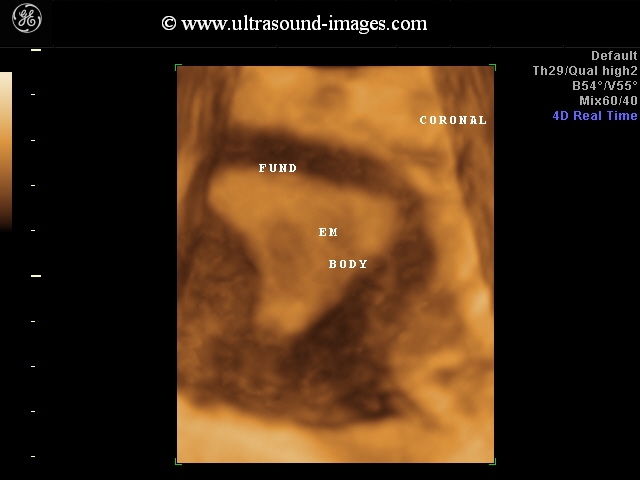
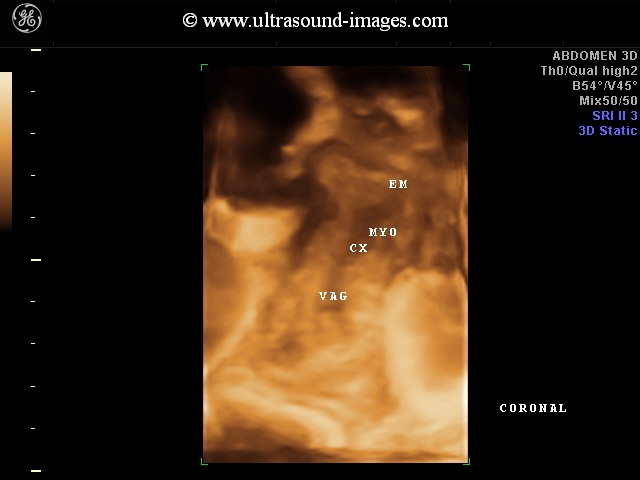

These 3-D ultrasound images show the normal endometrium of the uterus from the fundus to the cervix. The vagina is also visualized towards the bottom of the 3-D ultrasound images. These images reveal a coronal plane through the uterus, perhaps the best view to appreciate the internal architecture of the uterus.
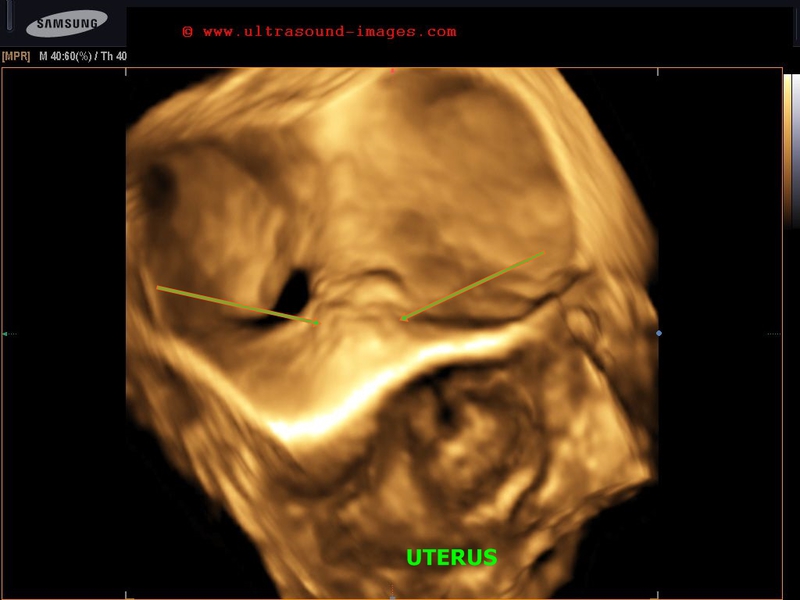
3D-ultrasound images septate uterus
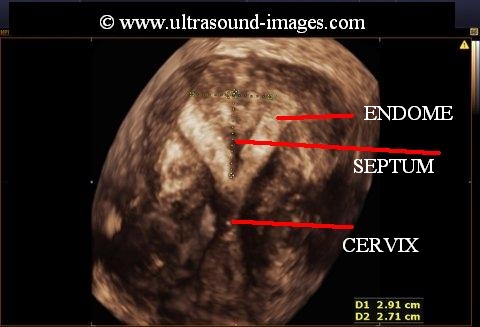

This uterus (see 3D ultrasound images above), show a coronal section through the organ, revealing a large septum passing through the centre of the uterus dividing the uterine cavity into two halves. The septum is seen merging with the myometrium above in the fundus. However, unlike bicornuate uterus, these 3D ultrasound images (of septate uterus) show the two halves or cornu are connected by myometrium without a gap between the two parts of the uterus.These 3D ultrasound images of septate uterus are courtesy of Dr. Arun Mahajan, MD, India.
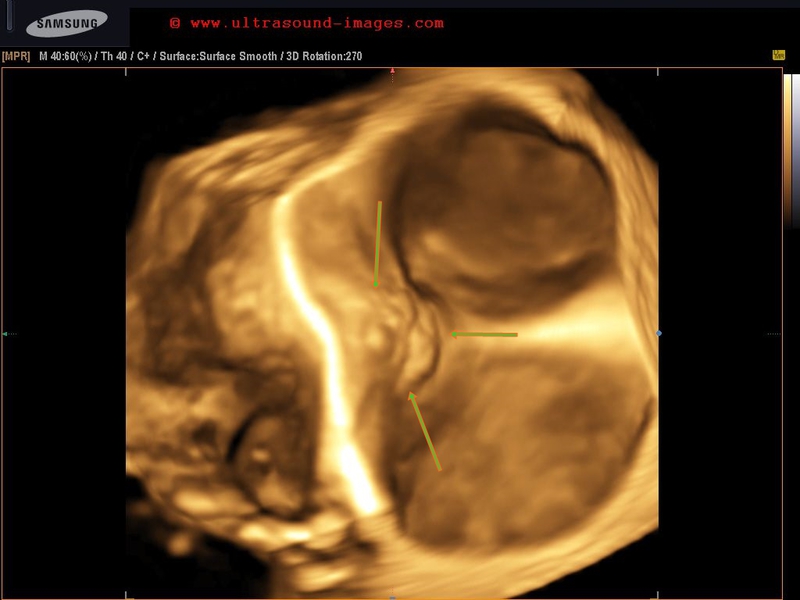
subseptate uterus with pregnancy

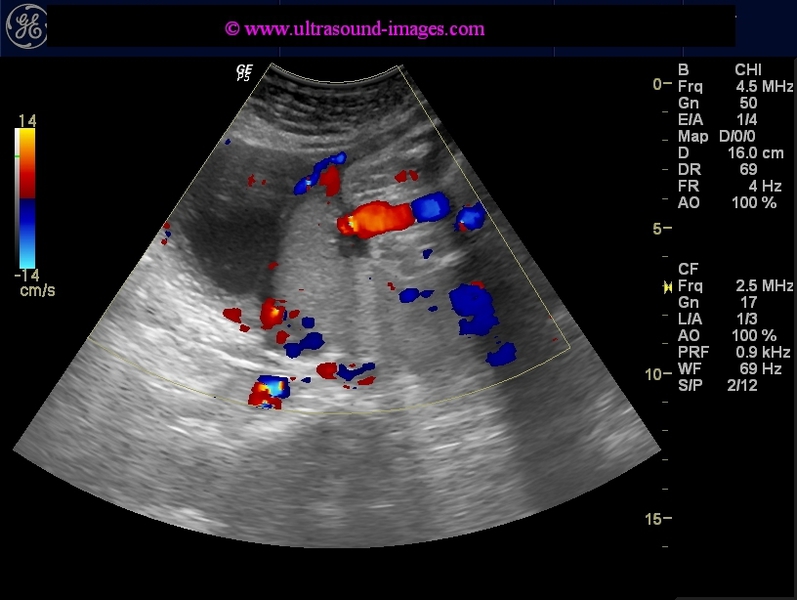
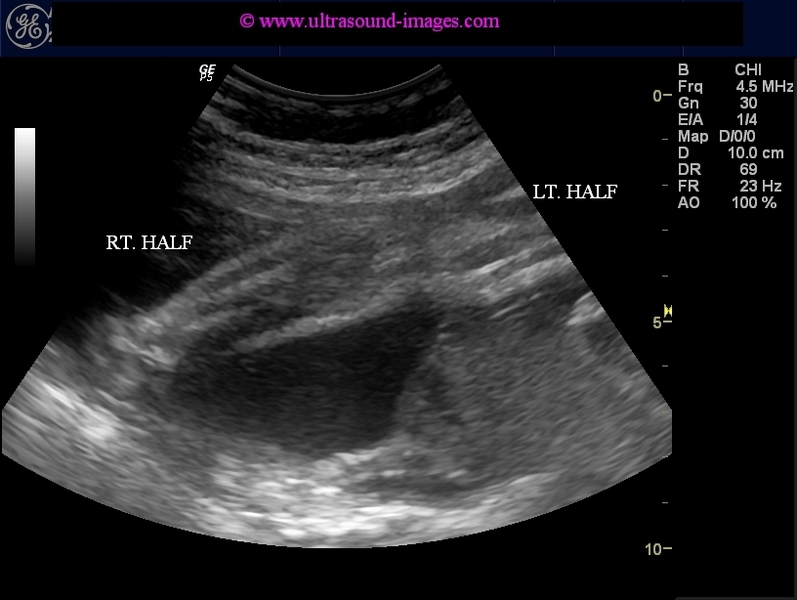

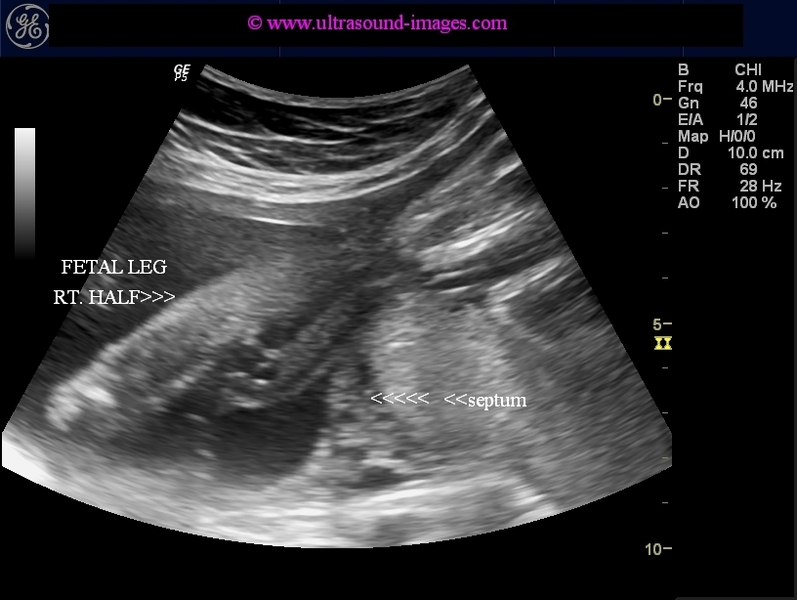
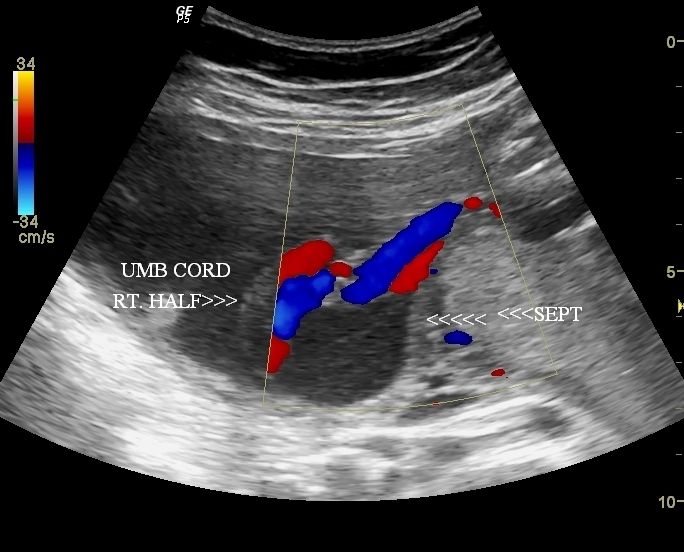

This is a third trimester pregnancy - 32 weeks with a partial septum in the fundus of the uterus dividing the uterus into a small right compartment and a large left one. The fetus occupies the
left half of the uterus with part of the legs and umbilical cord in the right compartment. These ultrasound images suggest pregnancy with subseptate uterus as the septum is incomplete and does
not reach up to the internal os.
a septate or subseptate uterus is associated with increased incidence of premature delivery and also abortions. However most cases of septate uterus or subseptate uterus may have no difficulty
conceiving.
References:
Subseptate uterus with pregnancy
septate uterus- 3D images case-2


Another fine example of septate uterus, brought out nicely by 3D ultrasound imaging. This 3D ultrasound study of septate uterus is courtesy of Dr. PK Srivastava, MD, India.
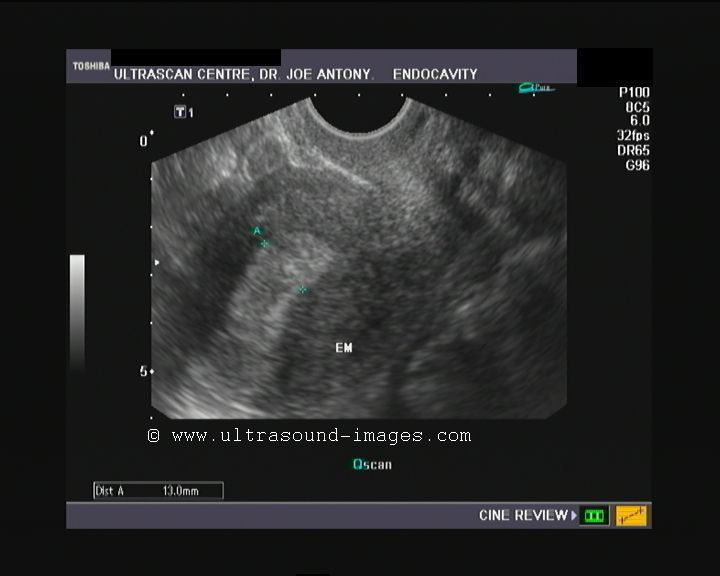
multiple polyps of the endometrium

These images of the uterus show multiple endometrial polyps, ( three are visualised). endometrial polyps are seen as small nodules or projections into the lumen of the endometrial cavity. These ultrasound images show the endometrial polyps to be echogenic, well defined and most importantly showing a vascular pedicle with the feeder vessel supplying the polyp on colour Doppler. Submucosal fibroids on the contrary, are larger, being more than 2 cm in size, and are usually hypoechoic. The absence of a single prominent feeder vessel in a submucosal fibroid, is another diagnostic feature, that distinguishes a submucosal fibroid from an endometrial polyp.
In this case study, the endometrial polyps are outlined by fluid within the endometrial cavity. In the absence of such fluid, sonohysterography, can be performed with injection of fluid into the endometrial cavity producing of fluid contrast, outlining the polyps.
These transvaginal ultrasound images of multiple endometrial polyps are courtesy of Dr. Gidda Ramaiah, MD, India.
References:
ultrasound imaging of the endometrium- RSNA
3-D ultrasound images of endometrial polyp



3-D ultrasound can highlight and better image the presence of even a very small polyp of the endometrium. These 3-D ultrasound images taken via the transvaginal route show the presence of a large endometrial polyp protruding into the endometrial cavity. These images are courtesy of Dr. Gunjan Puri, MD
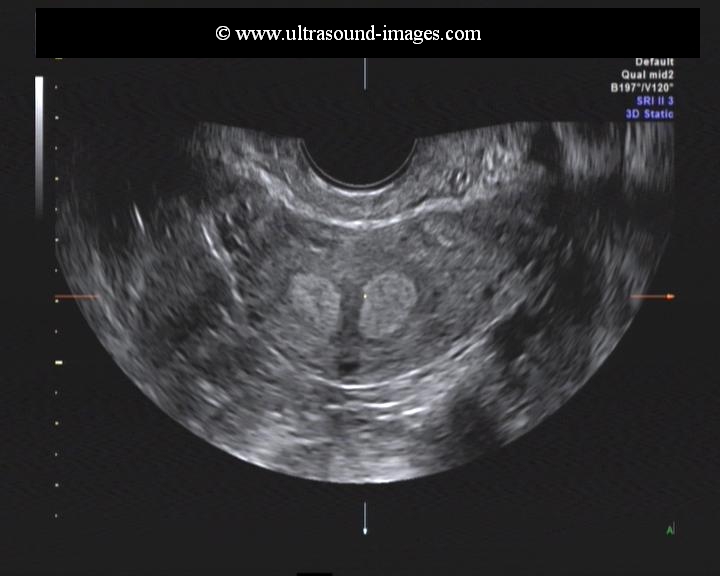
3-D ultrasound bicornuate uterus with non communicating horn

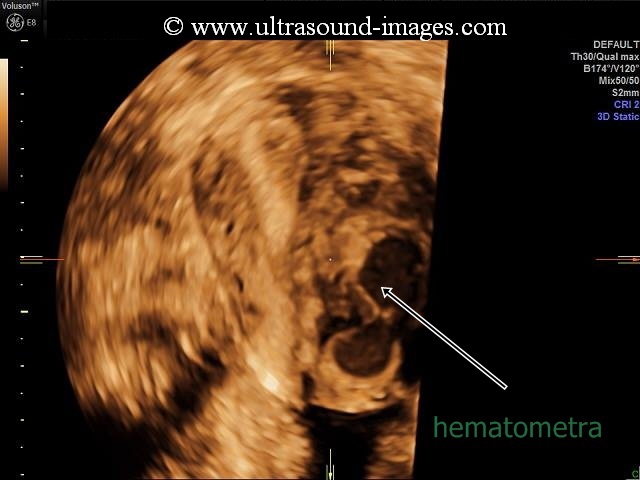

This patient has a bicornuate uterus with the left horn not communicating with the cervical canal. The result is the collection of menstrual blood within the non-communicating left horn of the bicornuate uterus resulting in hematometra. Lack of drainage of the hematometra can result in an endometrioma or even endometriosis as the blood seeps into the uterine walls and sometimes into the pelvic cavity. The 3D ultrasound images above (courtesy of Dr. Mayank Chowdhury, MD) demonstrate the bicornuate uterus with non communicating left horn with resultant hematometra and possibly an endometrioma of the uterus.
References:
Bicornuate uterus with non cmmunicating horn of uterus
hydrosalpinx-fallopian-tube




This middle aged female patient had history of left-sided pelvic pain. Ultrasound images show a narrow, serpentine tubular fluid filled structure which is anechoic with thin walls. This tubular structure is in close relation to the left ovary and yet separate from it, thus ruling out an ovarian cyst. Further, incomplete septae are present within this tubular structure. This gives the appearance of a cogwheel structure within this tube. All these findings suggest fluid filled, dilatated left Fallopian tube or hydrosalpinx. These ultrasound images of hydrosalpinx are courtesy of Ravi Kadasne, MD.
Among the common causes of hydrosalpinx are:
Endometriosis with the resultant stricture or narrowing of the fallopian tube resulting in fluid accumulation within the affected fallopian tube. Hydrosalpinx can also be caused by tubal ligation and past history of ectopic pregnancy within the fallopian tube. Hysterectomy can also produce a hydrosalpinx if the Fallopian tubes are not surgically removed as in cases wherein the tubes are maintained to prevent damage to the ovarian vessels. ovulation induction as well as malignant masses involving the fallopian tubes can also produce a hydrosalpinx. Pelvic inflammatory disease is also a very common cause of hydrosalpinx.
Complications of a hydrosalpinx:
One of the most dreaded complications of a hydrosalpinx is purulent infection of the affected Fallopian tube resulting in a condition called pyosalpinx. This is characterized by pyogenic matter within the fluid filled Fallopian tube giving rise to echogenic particles within the fluid. Another complication which can give rise to an emergency is torsion of the fluid distended Fallopian tube.
References:
sonographic imaging of hydrosalpinx- sonoworld article
3D-ultrasound-copper-T-IUCD
These 3D ultrasound images of a Copper-T IUCD or IUD (intrauterine contraceptive device) courtesy of Dr. Mayank Chowdhury, MD, India show the ease and clarity of imaging of the copper T after its insertion. The copper T is seen in the in first image as an echogenic linear object with two arms. The second image shows it as a sonolucent area (also in 3D).
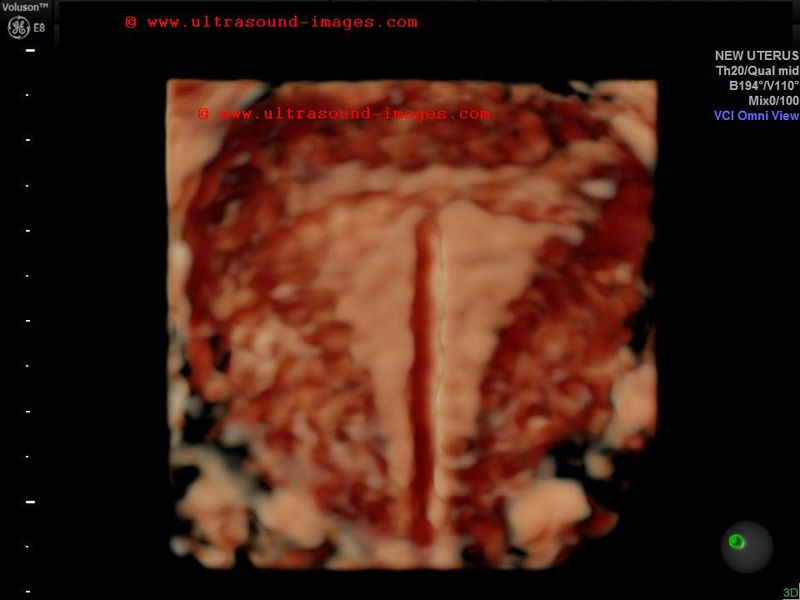
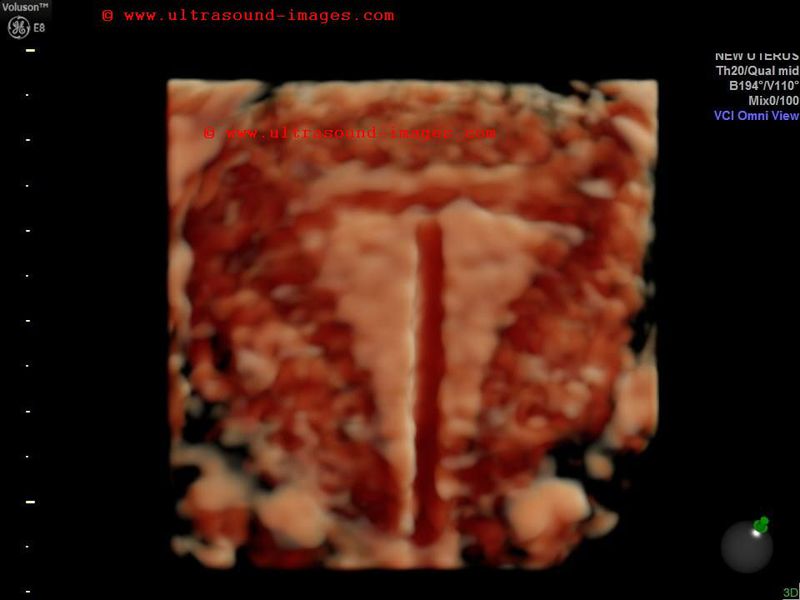
congenital-anomaly-rudimentary-horn-of-uterus
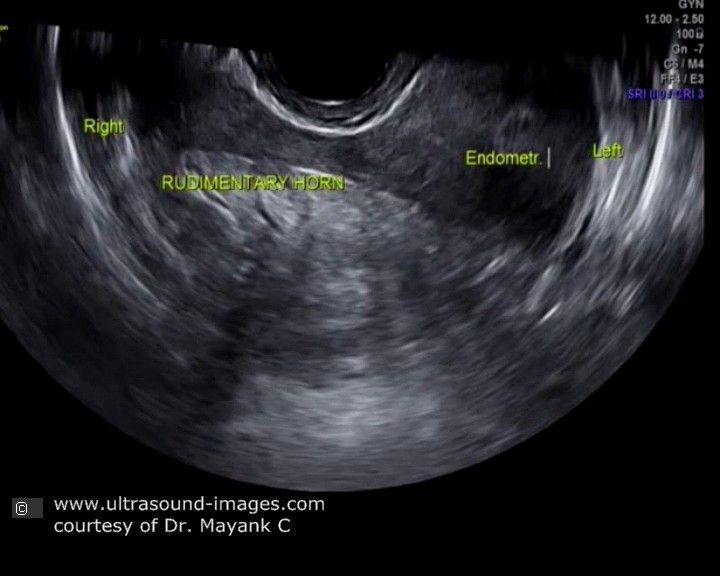
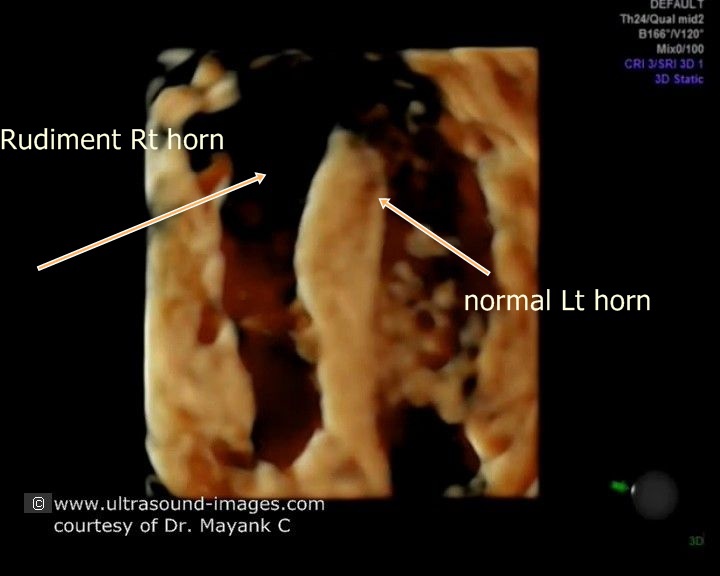
These 2-D and 3-D ultrasound images of the uterus show a relatively rare congenital anomaly of the uterus where the right horn or cornu of the uterus is hypoplastic giving rise to what is known as a rudimentary right horn of the uterus. Such an anomaly is also known as a variant of Mullerian dysgenesis. this congenital anomaly of the uterus, rudimentary horn is best diagnosed by 3-D or 4-D ultrasound imaging as shown above. Rudimentary horn of the uterus may have one of several variants- 1)absence of endometrial cavity in the rudimentary horn 2) presence of cavity in the rudimentary horn of the uterus 3) communicating or non-communicating cavity of the rudimentary horn. Often it may be difficult to exactly in point the subtype of rudimentary horn of the uterus. In this case, the rudimentary horn of the uterus on the right side appears to have an endometrial cavity but it is doubtful if it communicates with the rest of the uterus. The left horn of the uterus appears to be normal in size and shape and hence there is a good chance of conception in this normal half of the uterus. these 3-D and 4D ultrasound images and video of right rudimentary horn of the uterus are courtesy of Mayank Chowdhury, MD.
References:
1) sonography of congenital anomalies of the uterus (sonoworld article)
2) imaging of congenital malformations of the uterus- Medscape article
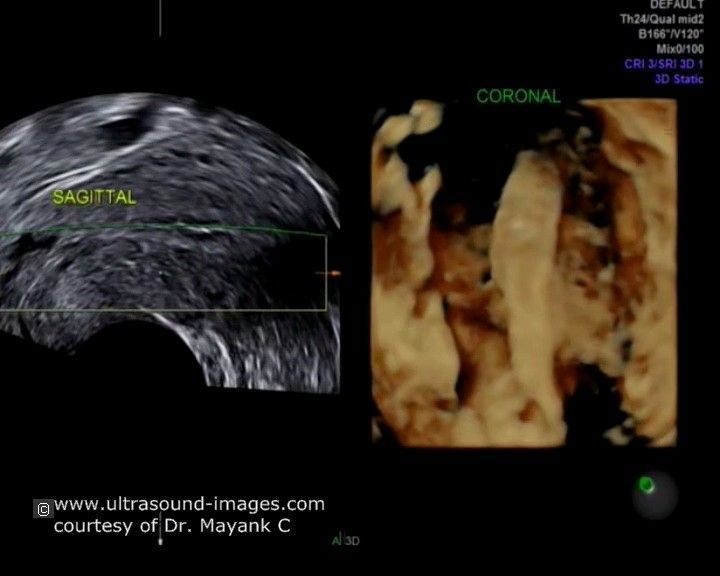
endometrial-cast-cervix
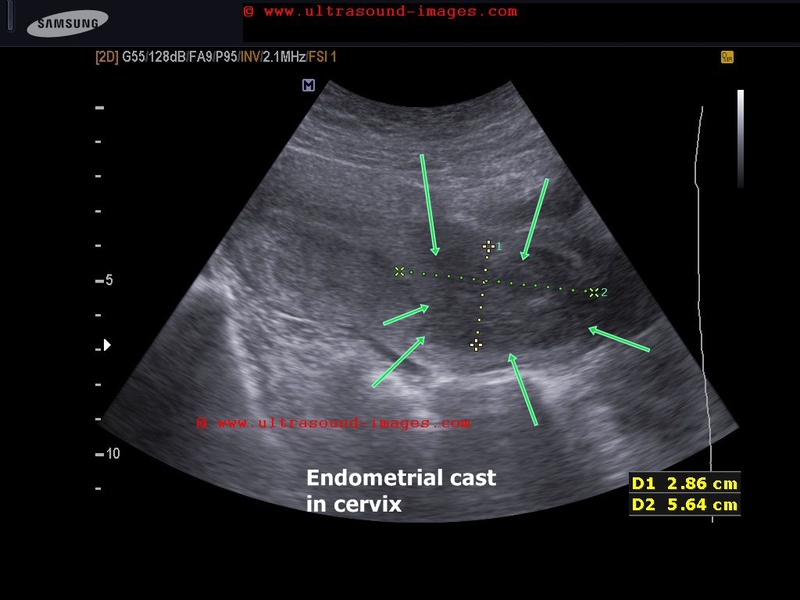
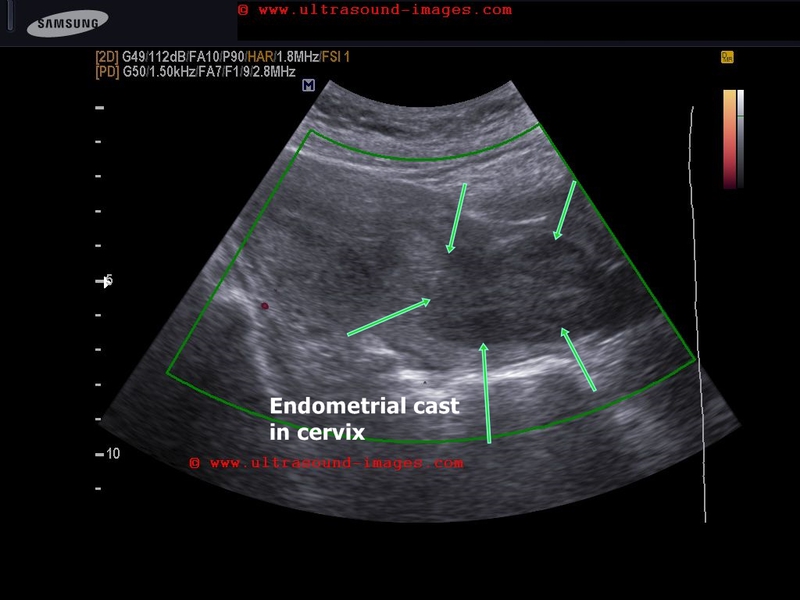
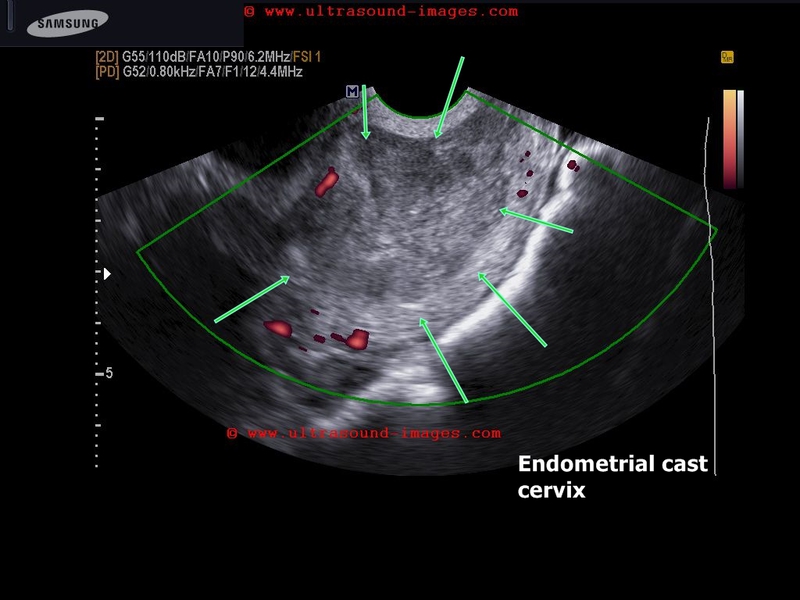
Large fleshy mass in cervix in a middle aged lady with heavy bleeding during menses.
Ultrasound shows a hypoechoic, fleshy non vascular mass in the cervical canal suggesting either blood (hematoma) or an endometrial cast.
The mass was expelled per vaginum and proved to be an endomtrial cast.
Endometrial cast is a fleshy endometrial tissue expelled during heavy menstrual bleeding usually due to progesterone use in non pregnant women.
References: endometrial cast what is it
unicornuate-uterus-3D-ultrasound


Ultrasound images above- 3D transvaginal scan show absent left horn of uterus. The right horn is visualized. s/o unicornuate uterus. Images courtesy of Dr. Wahid Majrooh, Afghanistan.
Endometrial-junctional-zone-contractions
retained-products-ultrasound-video
Retained products of conception:
- following D&C to terminate a 2nd trimester pregnancy
- multiple fetal bony fragments seen in uterine cavity
-ultrasound video above (courtesy Dr. Mohummed Atoom, Jordan) shows multiple echogenic foci within endometrial cavity
- bony pieces are removed by hysteroscopy
cervical-hydrops-stenosis
Hydrosalpinx



Ultrasound Diagnosis of Hydrosalpinx
- Anechoic or Hypoechoic Tubular Structure: Fluid-filled, elongated, and folded structure in the adnexal region.
- Incomplete Septations: "Beads on a string" sign due to incomplete septa.
- Thin or Thick Walls: Chronic cases may have thicker walls.
- No Internal Vascularity: Color Doppler shows no flow within the fluid-filled tube.
- Surrounding Ovaries: Typically separate from the ovary.
- Unilateral or Bilateral: May affect one or both fallopian tubes.
- Possible Debris: If infected, echogenic debris may be present.
© 2026, Joe Antony, MD All images and content in this site are copyrighted. www.ultrasound-images.com When visiting this site, we may use cookies to improve the performance of this site. Use of this site means you accept the use of cookies. Read our privacy policy at this page: https://www.ultrasound-images.com/privacy-policy/