
Ultrasound images of Ureteric calculi
Contents of this page
- Pelvi-ureteric junction calculus
- Multiple calculi in lower ureters
- 3-D Ultrasound image of Vesico-ureteric junction calculus
- VUJ calculus and its effect on ureteral jet
- Mid ureteric calculus
- Grades of hydronephrosis (on Ultrasound imaging)
- Complications of hydronephrosis
- Case-2: Pyonephrosis with ureteric calculus
- Hydronephrosis of lower moiety of duplex kidney
- another example of mid ureteral calculus
- distal ureteric calculus
- graded compression for ureteral calculi
- 3D-fly-through-ureter-ultrasound-video
- Distal Rt ureteral calculus-2
Pelvi-ureteric junction calculus
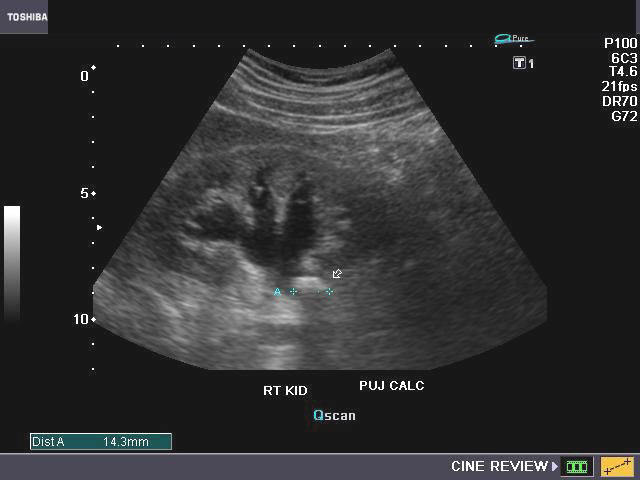

PUJ stone or UPJ stone
This patient had pain in the right lumbar region. Sonography of the abdomen showed hydronephrosis of the right kidney with a moderately large calculus (14mm.) at the right Pelvi-ureteric junction (arrows). Such calculi cause partial obstruction of the renal pelvis and may cause severe ureteric colic. Ultrasound images of pelvi-ureteric junction calculus, were taken with a Toshiba Nemio-XG ultrasound machine. (Synonyms: PUJ calculus or UPJ calculus or UPJ stones).
Reference:http://www.jultrasoundmed.org/cgi/reprint/27/10/1441(free article and images)
Multiple calculi in lower ureters

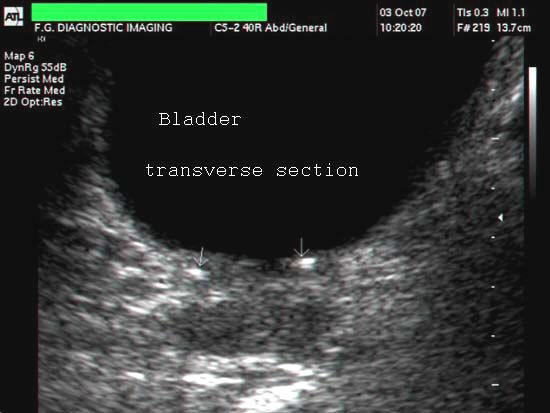
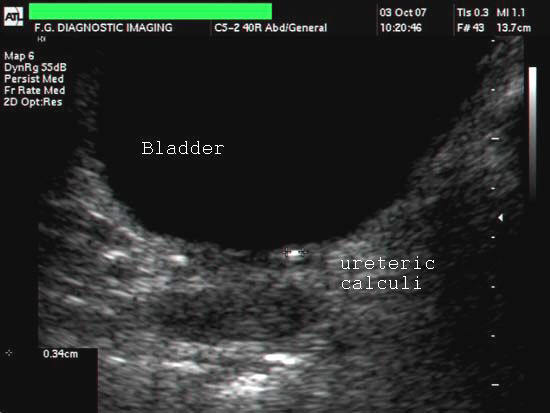
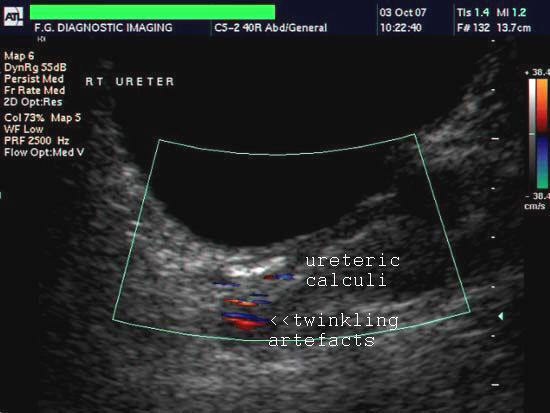
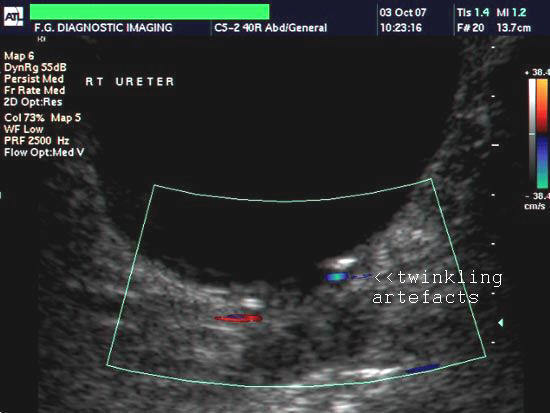
The above ultrasound images show multiple, small calculi (3 to 4 mm. in size) in both ureters. Color doppler imaging shows twinkling artefacts posterior to the calculi. There is mild dilation of the right ureter. Ultrasound images taken with an ATL ultrasound machine, courtesy of Mr. Shlomo Gobi, Israel.
3-D Ultrasound image of Vesico-ureteric junction calculus
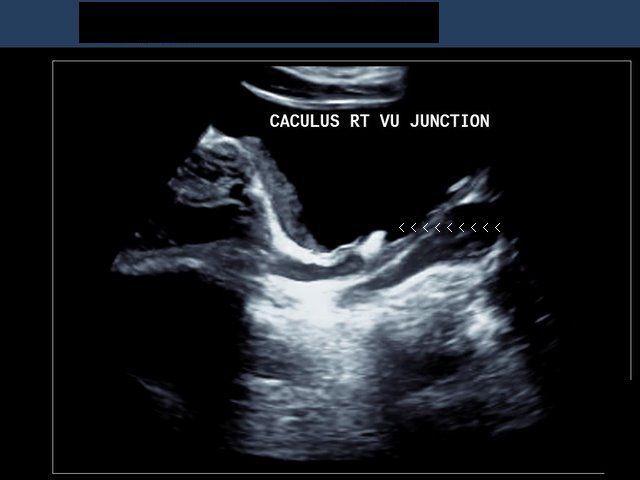
3-D sonography of ureteric calculi.
This 3 D ultrasound image shows a calculus lodged at the distal end of the right ureter at the vesico-ureteric junction (arrowheads). 3-D imaging leaves little to the imagination in such cases. Ultrasound image taken using a Philips IU-22 ultrasound system, by Dr. Ravi Kadasne, UAE.
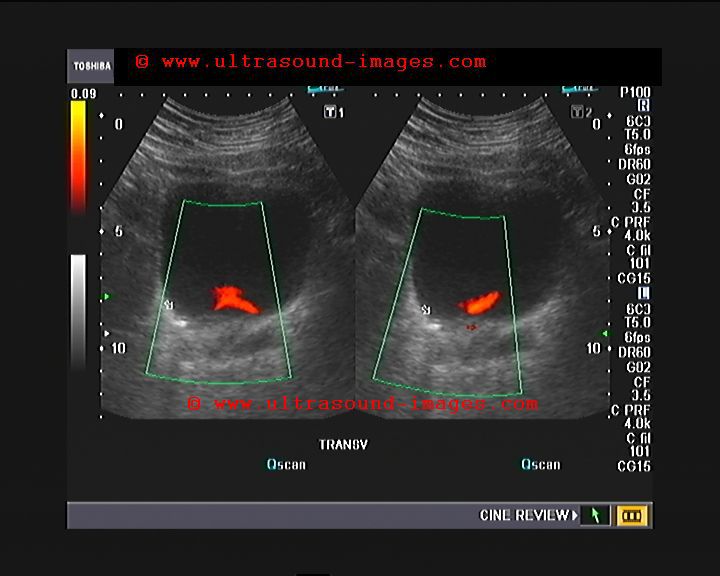
VUJ calculus and its effect on ureteral jet
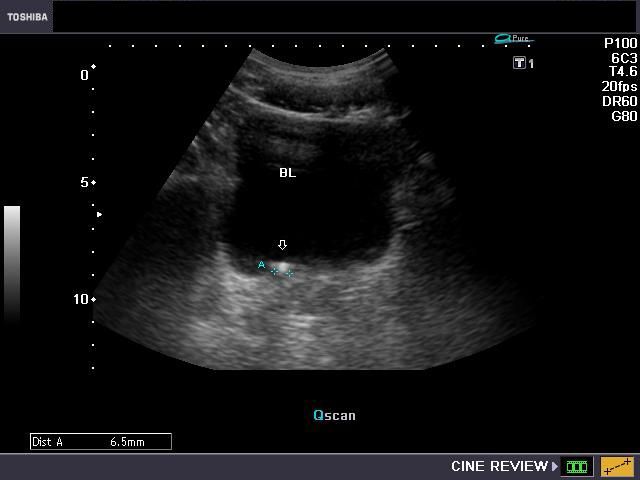
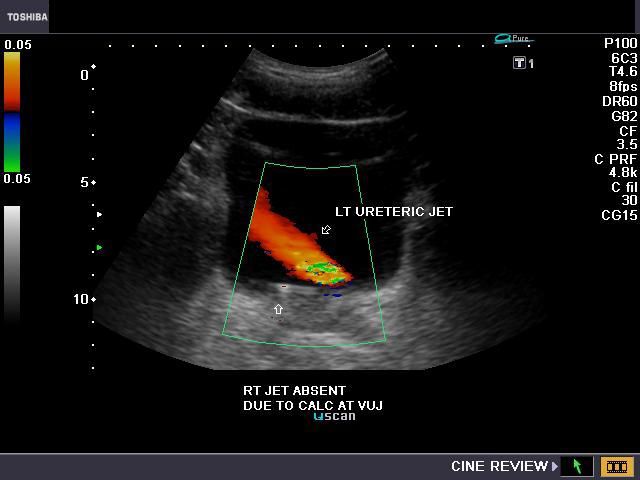
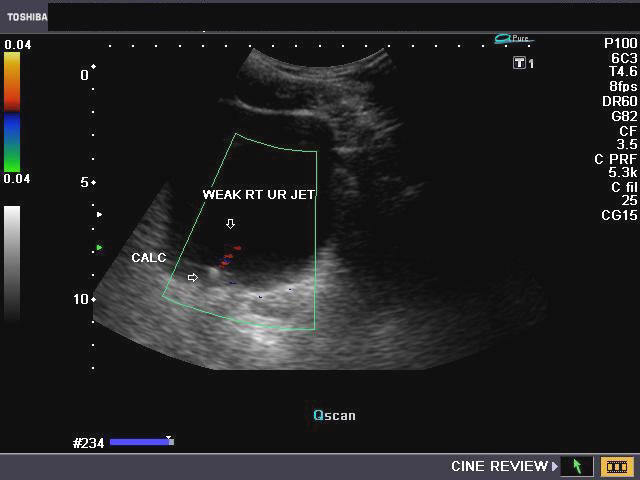
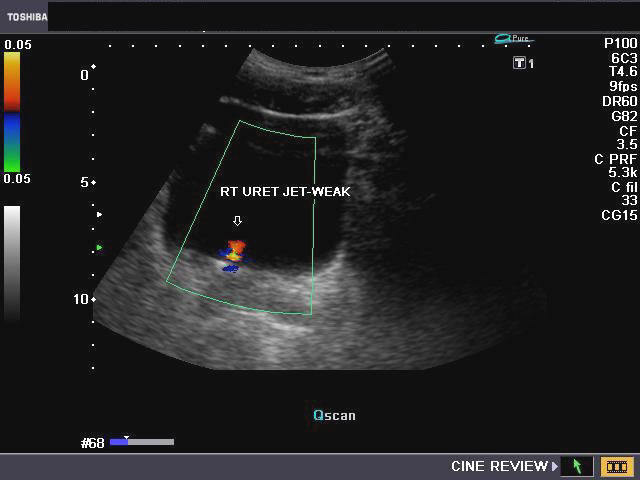

This was a young male patient with right ureteric colic. Sonography of the pelvis shows a small right Vesico-ureteric junction calculus of 6 mm. Color Doppler evaluation of the urinary bladder showed multiple and frequent powerful left ureteric jets of urine (see color Doppler image- topmost row-right). However the right ureteral jet was weak and far less frequent. The right kidney showed mild hydronephrosis. This means that there was partial right ureteric obstruction as a result of the stone.
Reference:http://www.ajronline.org/cgi/reprint/159/4/773.pdf
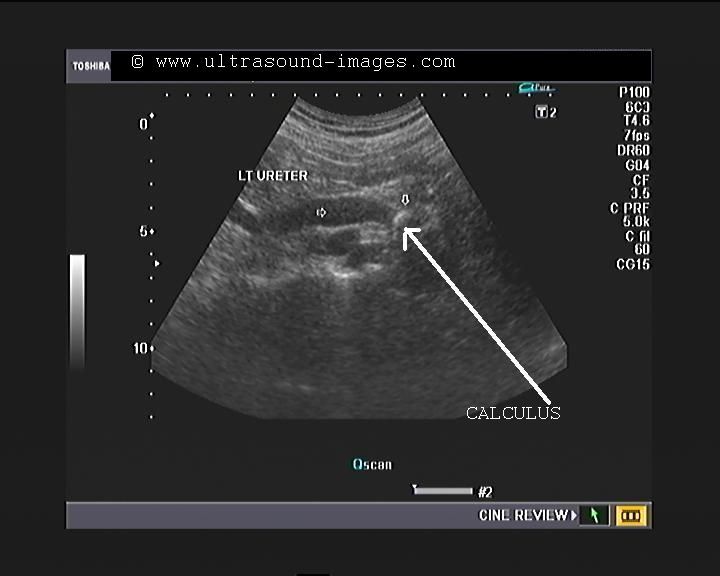
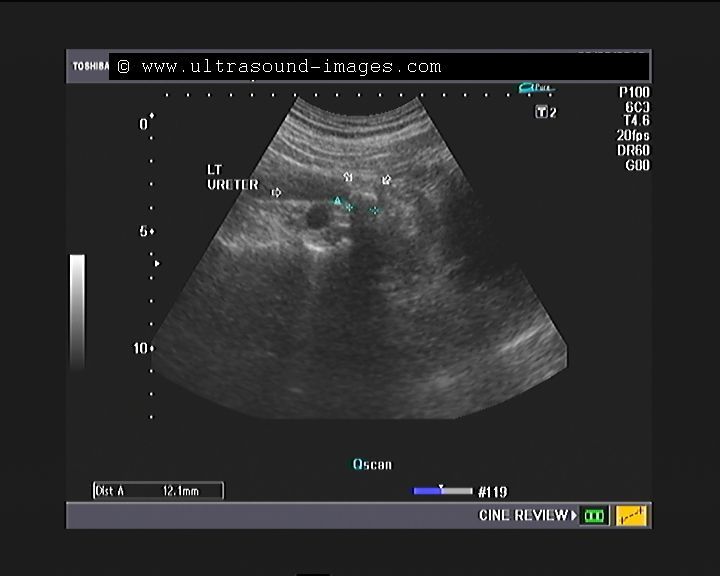
Mid ureteric calculus



(Calculi or stones in the mid ureter).
This patient had severe pain in the left lumbar region. Sonography of the left kidney and ureter shows moderately severe hydronephrosis in the affected kidney (ultrasound image top- left). The other ultrasound images show marked left hydroureter with dilation of the ureter till the level of the ureteric calculus. The stone in left ureter measures 1.2 cms. and causes severe backpressure changes on the upper urinary tract.
Grades of hydronephrosis (on Ultrasound imaging)
Physiological splitting of the renal pelvis
Images of fully distended urinary bladder

Mild splitting of the pelvis of left kidney
Physiological splitting of the left renal pelvis disappears after micturition
Physiological mild splitting of the left kidney is observed in the image on top- right. This apparently is the result of an over-distended urinary bladder with mild back pressure changes. On evacuating the bladder (post micturition ultrasound image), the left kidney appears normal. Transient splitting of the renal pelvis is a commonly observed phenomenon during sonography, and does not have significance if it disappears after micturition.
Reference: sonography of hydronephrosis
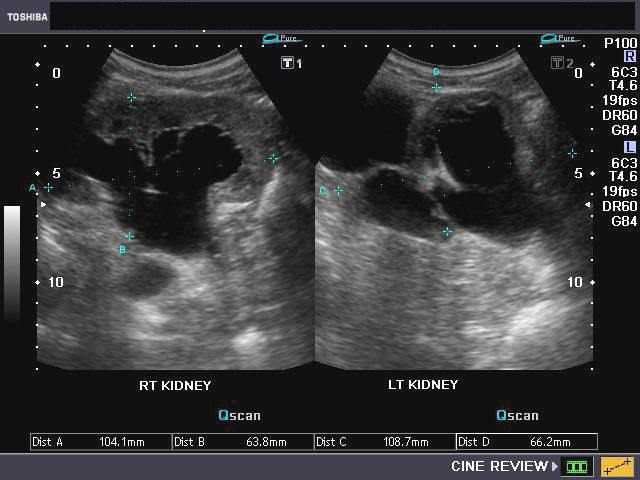
A) Mild hydronephrosis

This images shows mild dilatation of the pelvis as well as the calyces of the right kidney suggesting mild hydronephrosis. The left kidney also appears to be affected similarly. This must be differentiated from mild dilatation of the renal pelvis alone (called splitting of the pelvis), which is physiological and transient; this means that on emptying of the urinary bladder, this appearance should disappear.
B) Moderate hydronephrosis
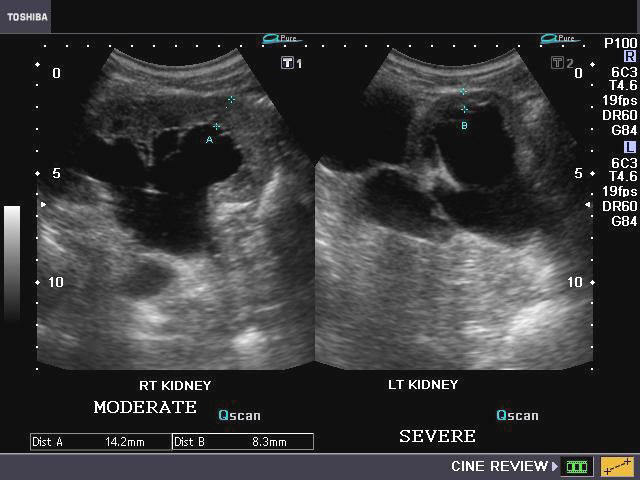
The above ultrasound images show cupping of the calyces with moderate dilation (Right kidney) of the pelvis and calyces. Despite the hydronephrosis the renal parenchyma is still preserved.
C) Severe hydronephrosis:
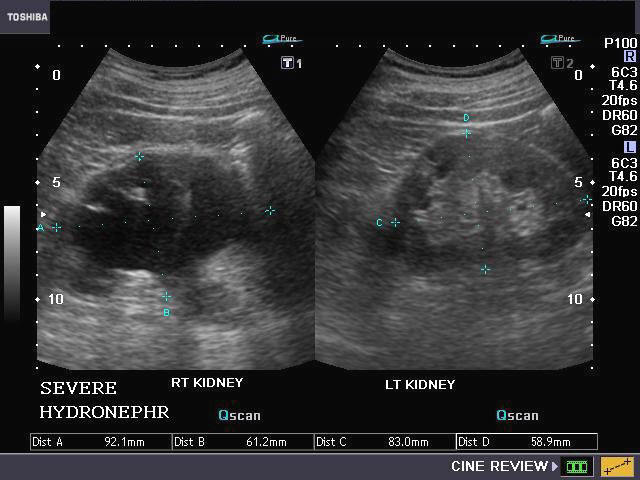

Case-2: severe hydronephrosis
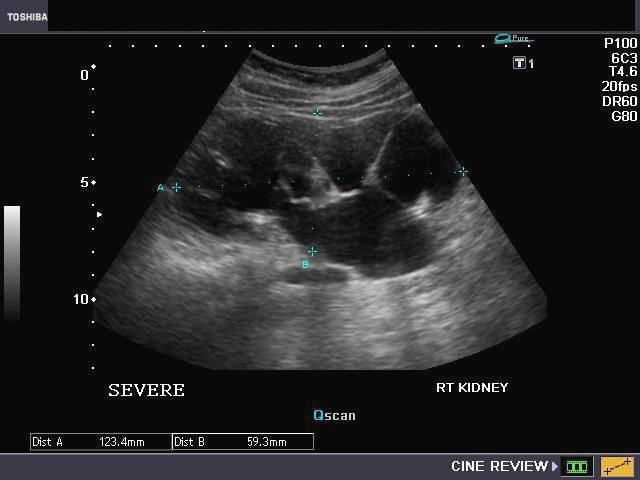
The above sonographic images show marked dilatation of the pelvicalyces with sever thinning of the renal parenchyma. In case-2, note almost total absence of normal renal tissue (cortex).
Reference:
http://emedicine.medscape.com/article/436259-diagnosis(free article)
http://knol.google.com/k/urinary-tract-obstruction#(free article)
Complications of hydronephrosis
Pyonephrosis
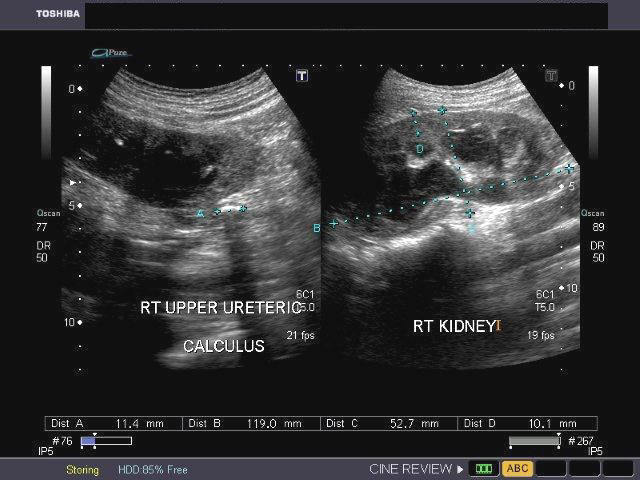
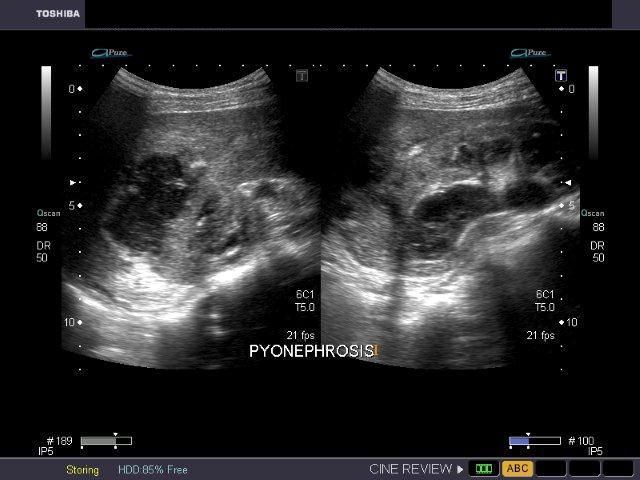
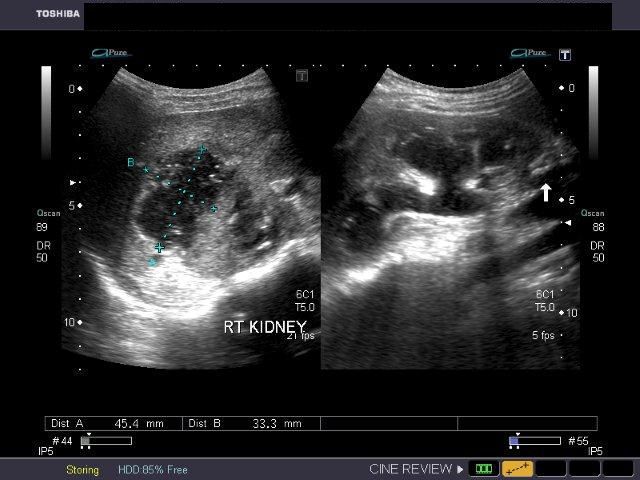
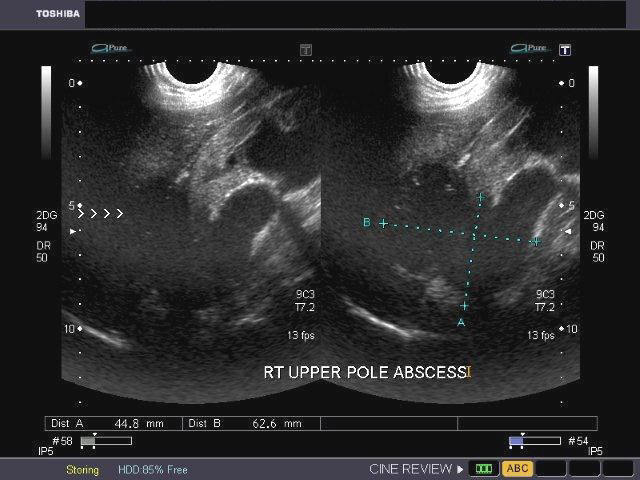
This patient showed a right upper ureteric calculus with obstructive changes in the proximal part of the right ureter and pelvicalceal dilatation. In addition, the right kidney also showed particulate debris within the dilated collecting system with breach of the upper pole of right kidney a large hypoechoic collection around this region suggestive of renal abscess formation. These ultrasound images suggest right pyonephrosis with abscess of right kidney. Chronic obstruction caused by the right ureteric calculus (see ultrasound image in top row- left), is the cause of this pathology, in this case. (Images are courtesy of Gunjan Puri, MD, India).
Reference: http://emedicine.medscape.com/article/440548-diagnosis
Case-2: Pyonephrosis with ureteric calculus
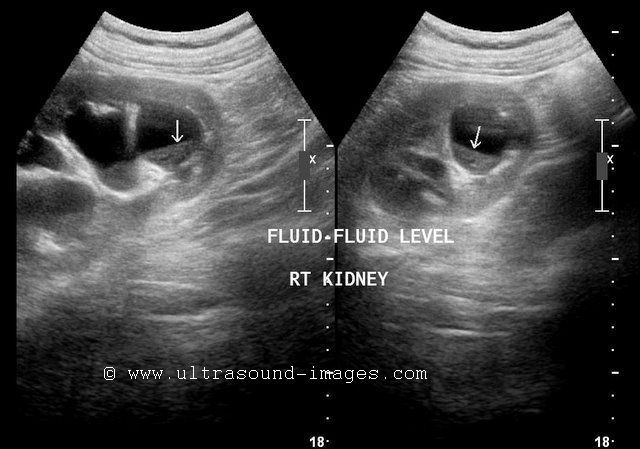
Ultrasound images of the right kidney show fluid-debris levels in the calyces as well as the pelvis of the right kidney. The pelvicalyces show moderate dilatation. There is also evidence of right hydroureter extending down to the lower third. Here a right ureteric calculus is seen (1.1 cms. in size). Final diagnosis- right pyonephrosis caused by right ureteric calculus. Ultrasound images are courtesy of Dr. Ravi Kadasne, MD, UAE.
Reference: http://www.ajronline.org/cgi/reprint/140/5/991.pdf
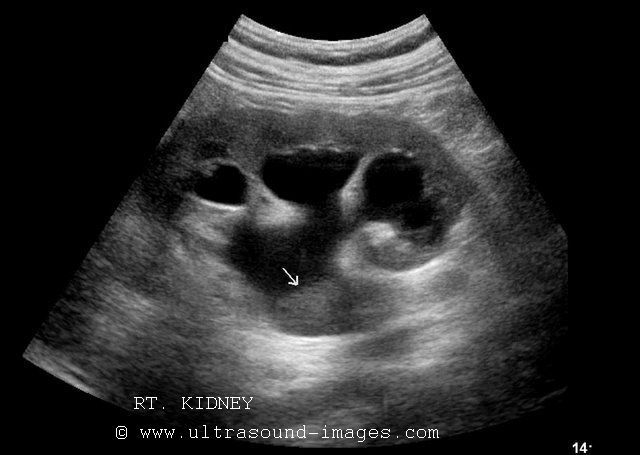
Hydronephrosis of lower moiety of duplex kidney


The above ultrasound images show a duplex kidney (duplication of the collecting system) with hydronephrosis of the lower half of the collecting system (lower moiety). This was caused by a calculus in the ureter from the lower half of the collecting system (lower moiety). Ultrasonography helps diagnose this pathology with much ease. The above images show presence of a kidney of greater length than its fellow with 2 separate echogenic renal collecting systems separated by normal renal parenchyma (this is the typical ultrasound appearance of duplex kidney). Images are courtesy of Ravi Kadasne, MD, UAE.
Reference: http://emedicine.medscape.com/article/378075-imaging
another example of mid ureteral calculus




this patient has a small calculus of just 6 mm in the middle third of the right ureter. However, the effects of the right ureteral calculus are obvious with moderate hydronephrosis of the right kidney.
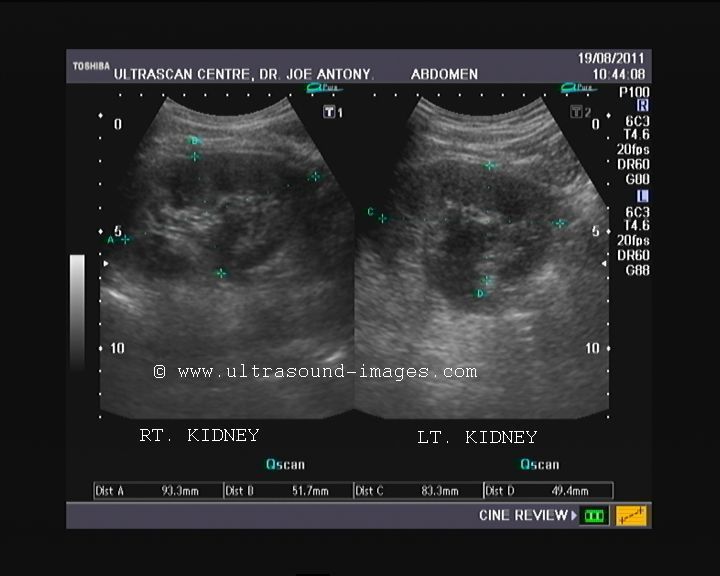
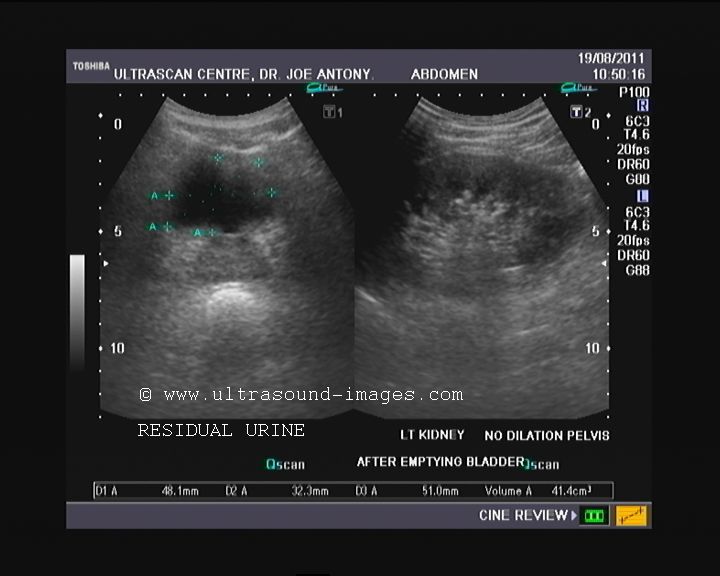
distal ureteric calculus


This young adult male patient had non-specific complaints with vague pain in both flanks. ultrasound imaging of the abdomen shows bilateral hydronephrosis with more severe changes in the right kidney. There is almost no functioning renal parenchymal in the right kidney with renal parenchymal thickness of just 0.5 mm.
The right ureter was poorly visualised, suggesting that this hydronephrosis of the right kidney may be due to Rt. pelviureteric junction obstruction. A calculus of 12 mm is seen in the dilated left ureter.
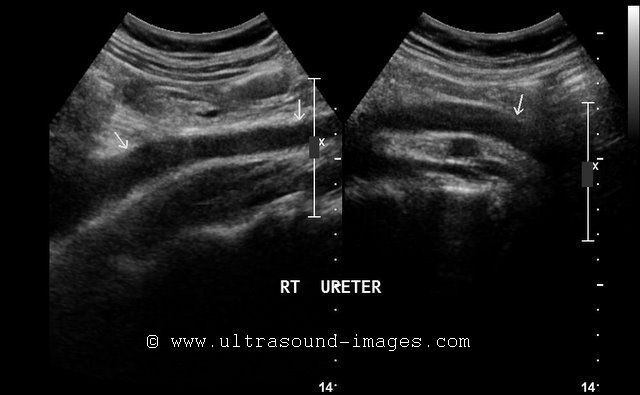
graded compression for ureteral calculi
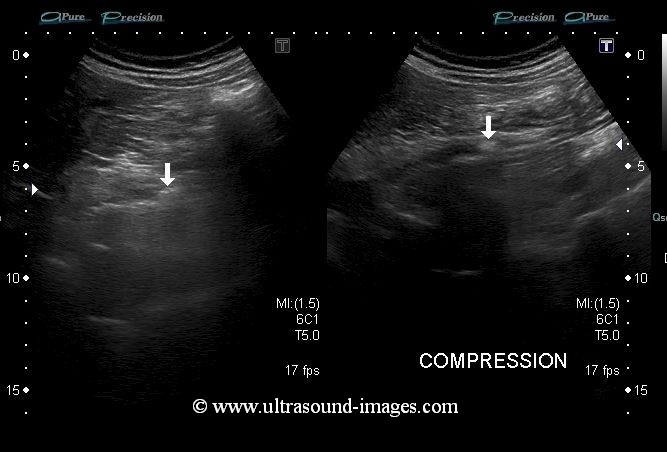
This image demonstrates graded compression as an excellent tool to visualize ureteral calculi. Graded compression involves gentle but firm compression over the region to displace bowel loops and their gas and feces to image the affected part- in this case ureteral calculi.
This ultrasound image (courtesy of Dr. Ravi Kadasne, MD, UAE) displays the effect of graded compression to reveal the ureteral (ureteric) calculus in full detail.
3D-fly-through-ureter-ultrasound-video
This 3D ultrasound video of the inside of a distended ureter shows a calculus lodged within its distal part. What is remarkable is the fly through view of the lumen of the distended ureter, where a virtual view of the ureter is possible almost as if flying through the tube. This ultrasound video fly through view is courtesy of Ravi Kadasne, MD, UAE.
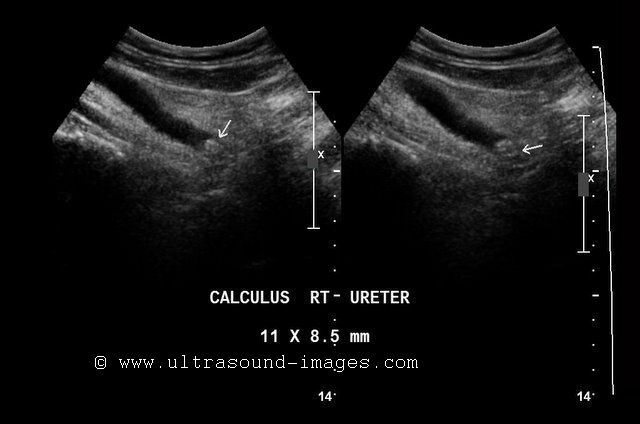
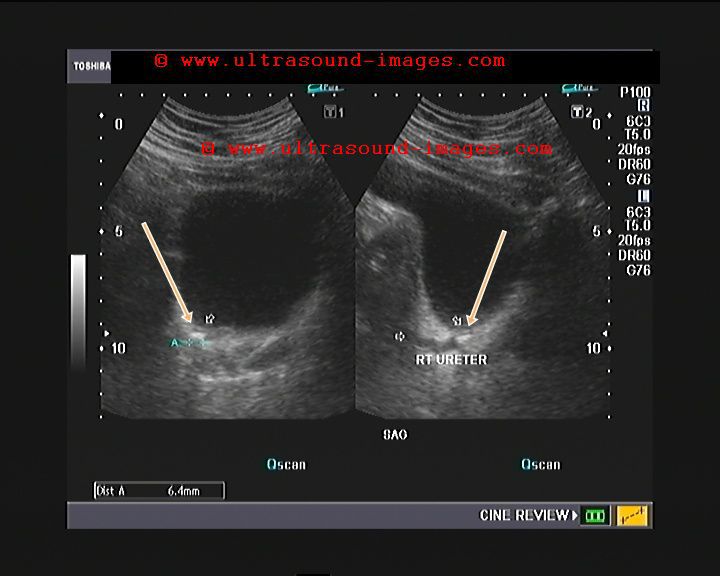
Distal Rt ureteral calculus-2
The distal Rt.ureter in this patient shows a 7 mm calculus lodged in the VUJ but which does not produce significant obstruction in this case. The color Doppler flow study shows normal Rt ureteric jet. CT scan of pelvis further confirms this finding.


© 2026, Joe Antony, MD All images and content in this site are copyrighted. www.ultrasound-images.com When visiting this site, we may use cookies to improve the performance of this site. Use of this site means you accept the use of cookies. Read our privacy policy at this page: https://www.ultrasound-images.com/privacy-policy/